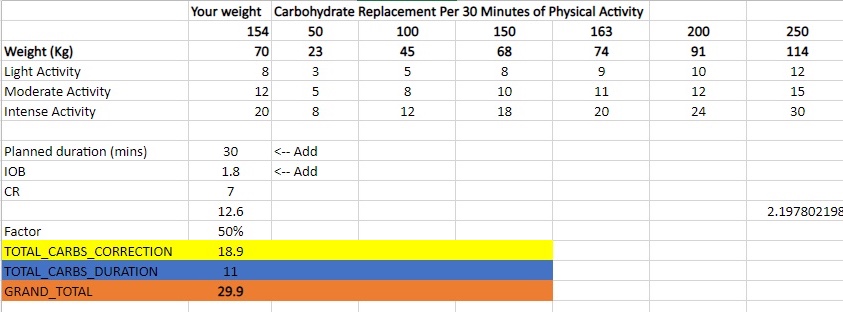
Before my run yesterday my blood glucose was lower than I felt was safe to start exercising (around 4 mmol/l ) despite reducing insulin to 70% of requirements and setting a higher temp target ( 7 mmol/l) an hour prior to exercising. I decided to eat an Anzac cookie (20g carbs) and accidently devoured some deep fried bread (30g of carbs). This was excessive to say the least ( I needed around 12g according to my calculator). It also created a complicated situation where I would need to inject prior to exercise or forego exercising all together and rather focus on injecting the appropriate amount of insulin (8.62 units) to counteract the carbs.
Factors to consider
As a rule of thumb I try to have as little insulin on-board as possible as this reduces the chances of hypoglycaemia (low blood sugar). Due to the carbs I ate I would now need to inject insulin prior to exercising or my blood glucose would rise excessively. I factored in that both fat (from the fried bread) and exercise would decrease the speed of digestion. Exercise decreases the speed of digestion as energy used for digestion would be diverted to my heart, lungs and muscles to fuel my activity and fat slows down gastric emptying and causes insulin resistance.
Insulin calculation
Utilising my IC ratio and exercise table I calculated I required around 1.7 units of insulin prior to the commencement of my run. I decided to be cautious and inject 1.5 units. I used a total of 4.4 units to return to euglycemia (normal blood sugar).
Insulin-to-carb ratio
carbs
Insulin Required
75%
50%
25%
20%
15%
5.8
50
8.62
6.47
4.31
2.16
1.72
1.29
Insulin calculation table
Table containing the amount of carbs I require for a specific duration of activity. This was derived from information found on the internet and my own experience.
Results
The results were by no means perfect, but at the very least I learned how much insulin I require and more or less when I should be injecting after I finish exercising. Its extremely difficult to predict how much exercise will amplify insulins activity, so it’s always safer to take a cautious approach.
My final decision was to inject 1.5 units prior to starting my activity and inject the remaining amount once my sugars started rising due to digestion resuming (around 35 minutes after stopping exercise).
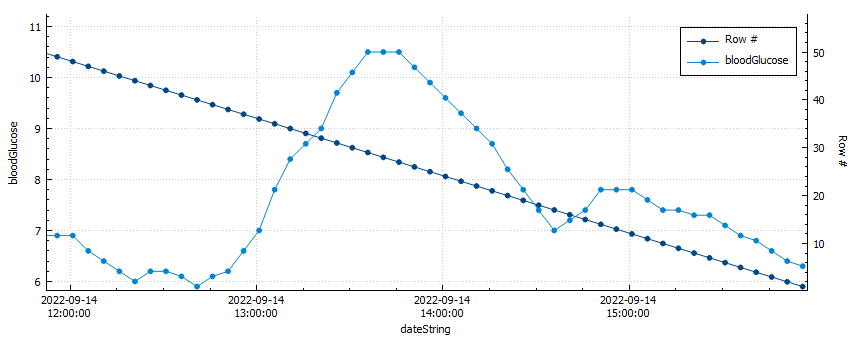
Blood glucose vs. row count
My blood sugar peaked at 10.5 mmol/l after only 1.5 units of insulin for 50g of carbs.
I used a total of 4.4 units of insulin (50% of the total insulin required) to return to euglycemia after my activity. My average blood glucose was 6.6 mmol/l and my time-in-range (TIR) was 100% for the duration of my activity.
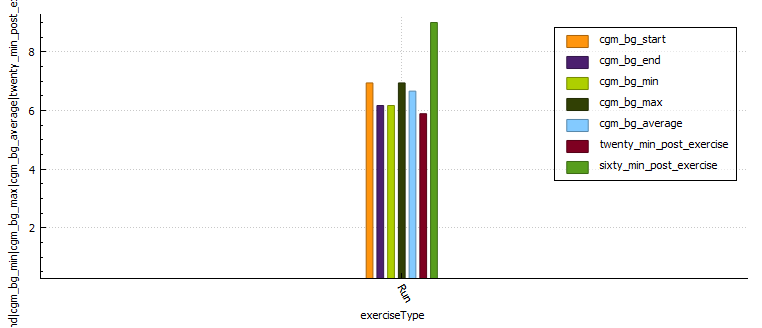
Graph with glucose control metrics during activity
Distance (km)
Moving time (minutes)
Average heart rate
Standard deviation
CGM BG start
CGM BG end
CGM BG min
CGM BG max
CGM BG average
Time in range
BG twenty minutes post exercise
BG sixty minutes post exercise
Lunch Run
4.92
29.53
170.2
0.308
6.94
6.17
6.17
6.94
6.66
100.0
5.89
9.0
Glucose control metrics
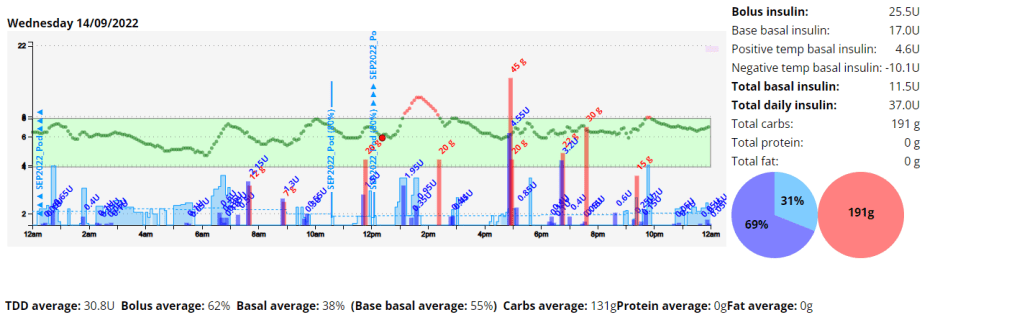
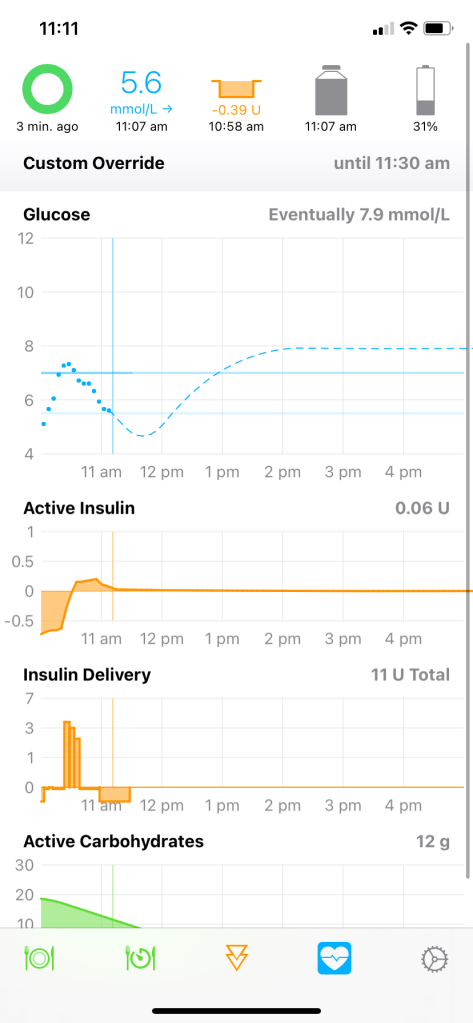
Daily overview graph with insulin and carbs.Diabetic management metrics.
My blood sugar control after exercise improved and I was happy with the results for the remainder of the day. Next time I would inject 20 minutes post exercise to prevent digestion resuming causing hyperglycaemia (high blood glucose).
The first week was challenging to say the least. As I have increased my physical activity my insulin needs seem to have fundamentally changed, and this resulted in quite a few lows. I also had some tech issues, my Android phone had an operating system error and my Dexcom sensor wasn’t enjoying the resistance training I was doing as it was inserted in my arm. I reached my activity goals but exceeded my diabetic and nutritional goals.
Body Metrics
Start
Week 1
Week 2
Week 3
Week 4
Weight (kilograms)
75.8
74
Body fat percentage (according to Samsung)
17.3%
Body fat percentage (according to the navy seal calculator)
15%
Total volume
Table stating the weekly body metrics I am tracking.
Exercise
Week 1
Week 2
Week 3
Week 4
Distance (kilometres)
25.17
Activity (hours)
6.24
Table stating the weekly exercise metrics I am tracking
Week 1 breakdown
Nutrition
Screenshot of the average and total macronutrients consumed during week 1.
Screenshot of average macronutrient consumed during week 1
Diabetes
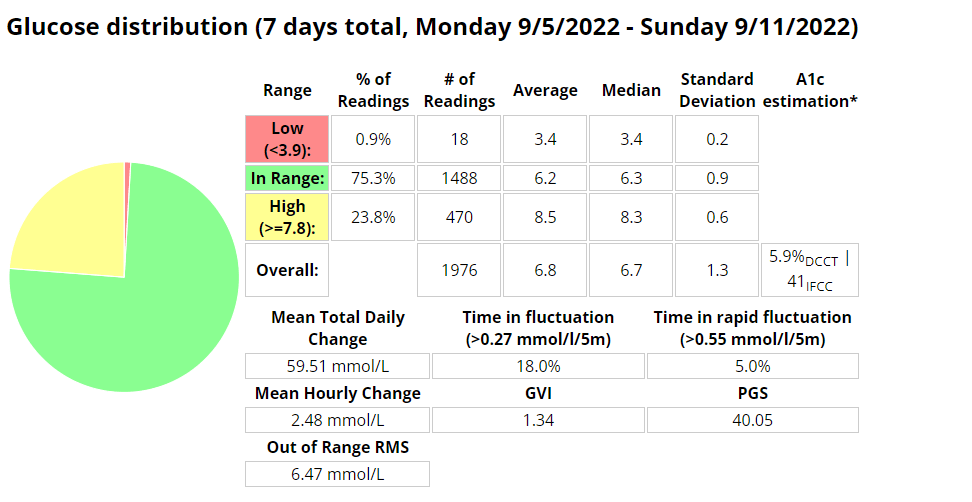
Ideally I want to see a time-in-range (TIR – 3.9-7.8 mmol/l) exceeding 90% with an average in the low sixes and a standard deviation (SD) around one (1).
It’s spring, and after a brief ‘almost two months’ of going off the reservation snacking at all times of day and barely exercising, I decided to check my weight. I discovered I had picked up a few kilograms since my last weigh in. After learning this, I decided that it was time for me to get my life back together and start another 30 day challenge. I find these great to provide the reason to get back into a routine.
I know that setting unrealistic goals (like losing 5kgs) isn’t going to work, so I’m going to break down my plan in to nutrition, exercise and diabetes goals.
Exercise
My plan for the month is to gym three days a week, run a minimum of 2 times per week and to mountain bike at least once a week. (So I guess I lied about setting unrealistic goals 🙂 )
Nutrition
For my meals I plan to stick to my usual low-ish carbohydrate meals during the week and try to only go coo-coo bananas on the late night snacking over the weekend. I’ll start carb-counting again as this will almost always yield the best results. This will be supplemented with 2-3 liters of water, depending on length of cardio that day.
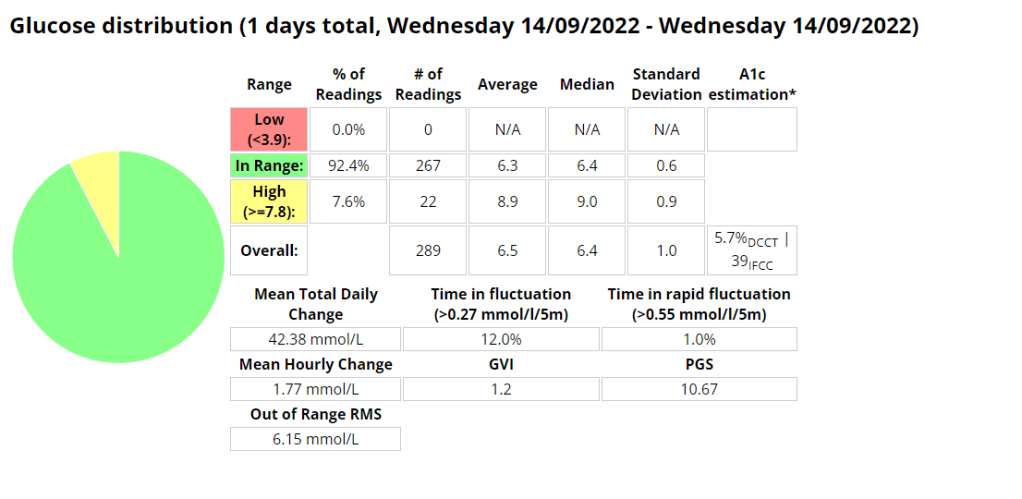
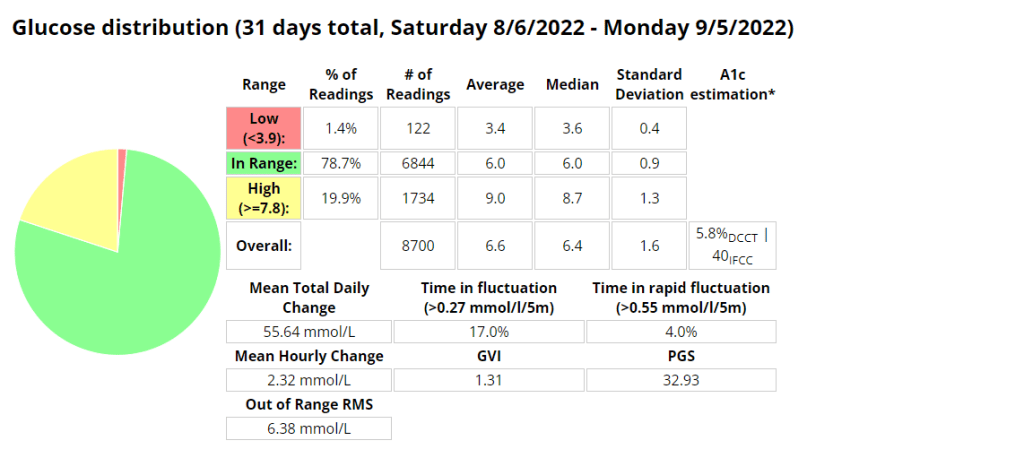
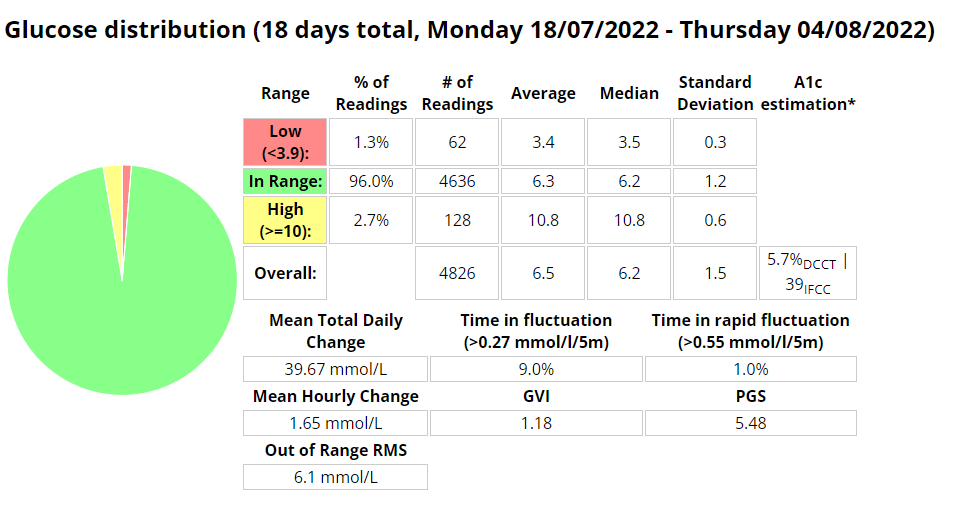
Diabetes
Above is a chart of my starting metrics. Lets see how quickly I can improve those values. Its going to be a little bit of an unfair test as I was not carb-counting during the above period.
We want to see the In range (Time-in-range) increase and the standard deviation decrease. By doing that the average and the A1c should follow. This will mostly be achieved by the diet component of the plan. The exercise component will allow me to eat more cabs and require less insulin, as well as improve circulation, sleep, blood pressure, mood, cholesterol, memory and overall mental and physical health.
I will check in with weekly updates to ensure I keep motivated and accountable.
Its only been a week and already I feel so comforted by the barely audible click of the pump depressing the plunger in the mini pump at meal times or sporadically throughout the day. Its the sound of blood sugar control. What a week its been learning all I can about Pod changes and being woken up on day 3 by the Pod alarm alerting me its 8 hours before the Pod expires. Once expired it was interesting to note that the Pod functioned as per normal, apparently for another 8 hours.
I had a Pod on days 3 and 4 that was inserted into my leg that may have had a cannula issue, as I struggled to maintain my standard level of control.
Its been a lot easier to exercise focusing on enjoying the task rather than if I would break the pump or rip out a cannula. Having no wires makes it a lot easier to run or gym as I don’t have to worry about pump placement as much. Previously I needed to ensure I had pants with pockets or a belt clip available.
I have also found sleeping a little easier, as I can barely notice the pump If I roll over onto it.
Flank insertion. Boost Omnipod – Time in Range (3.9 -7.8 mmol/l)Boost Omnipod – Time in Range (3.9 – 10 mmol/l)
Unannounced meals
I decided to test the system with unannounced meals consisting of 40g of carbs or less. I am a bit of a control freak when it comes to diabetes so I have been postponing testing this for a long time. The results were outstanding. I will be writing more about this in the future, including any automations I use or test.
Boost Omnipod – UAM – Time in Range (3.9 -7.8 mmol/l)
Boost Omnipod – UAM – Time in Range (3.9 – 10 mmol/l)
I recently posted about how my experimenting with running using AAPS was progressing. I observed that under certain conditions there was a significant lag between the capillary blood and CGM readings at about the 30 minute mark. This sparked some interest in wanting to know if I could predict what my capillary blood sugar could be using machine learning. I’m still not sure if its entirely possible yet, but I am having fun trying, and I have learned a lot in the process. I’m currently working on the script that will allow me to overlay a lot more AAPS data during a workout, including predictions.
I am getting a lot better at managing blood sugars as I noticed the last 14 exercises I was in range (3.9-7.8) 100% of the time.
Python script data capture
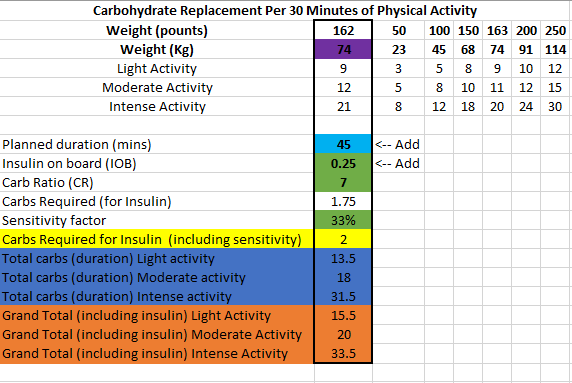
I have changed my approach slightly towards eating before exercise and have piggy backed off some research done by Gary Scheiner to create a spreadsheet that estimates the carbs required and effort for a run.
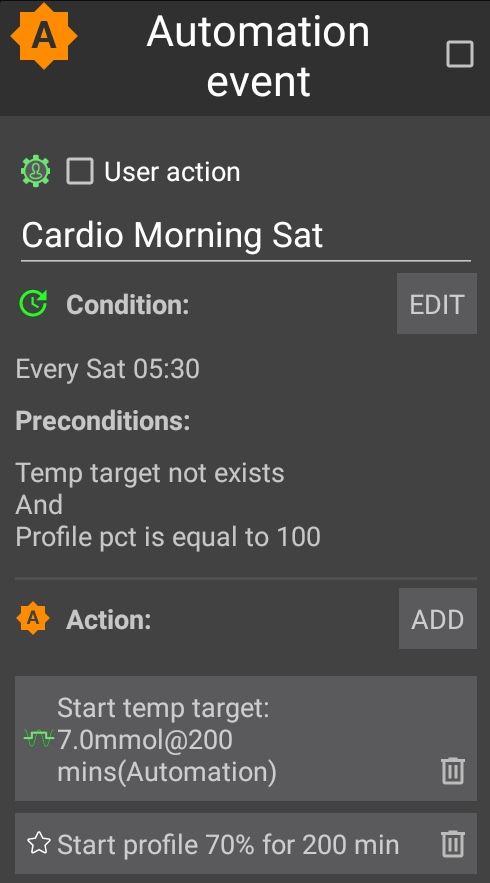
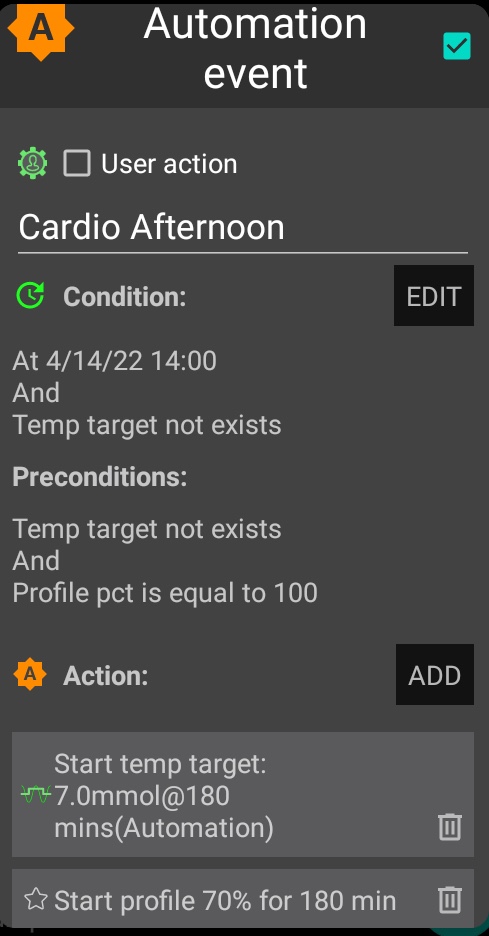
I decided to try using an automation to lower insulin levels and raise my glucose target before doing cardio. This allows AAPS to start this process at 05:30am on my days of choice so that my body is ready to exercise safely and with less need to consume carbohydrates. In my limited testing the process is working well, with some slight tweaking for testing parameters needed. NOTE: I only added half the amount of carbs I consumed to the APS for tracking. This is to avoid overcorrecting by the algorithm.
Expectations
I am trying to find the ideal conditions to exercise where I can experience moderate blood glucose fluctuations and not be required to consume large amounts of carbohydrates to keep me exercising safely. In the past on MDI I used to exercise fasted with only basal on board, which allowed me to stay in range for about 40 minutes before needing carbs. I am hoping to achieve this same amount using a pump. In past experiments I was able to achieve similar results during exercise by significantly reducing basal rates but I found that post exercise I struggled with higher than usual blood glucose readings for a few hours due to lack of insulin in my body.
Automations
Blood Glucose vs. CGM
The CGM results differed during exercise an average of 25% from blood readings. This made me decide to start some research of my own into using machine learning to try and estimate my blood glucose during exercise.
Results / observations
The automation route works well if you plan your exercise far enough ahead. The next experiment I will drop the profile percentage to 60% and observe. I noted an average of about 25% difference between the results the CGM and the finger pick tests. I was however able to keep my readings in range 100% of the time using 34g of carbs for the duration of the 50 minute experiment.
Capture from Nightscout
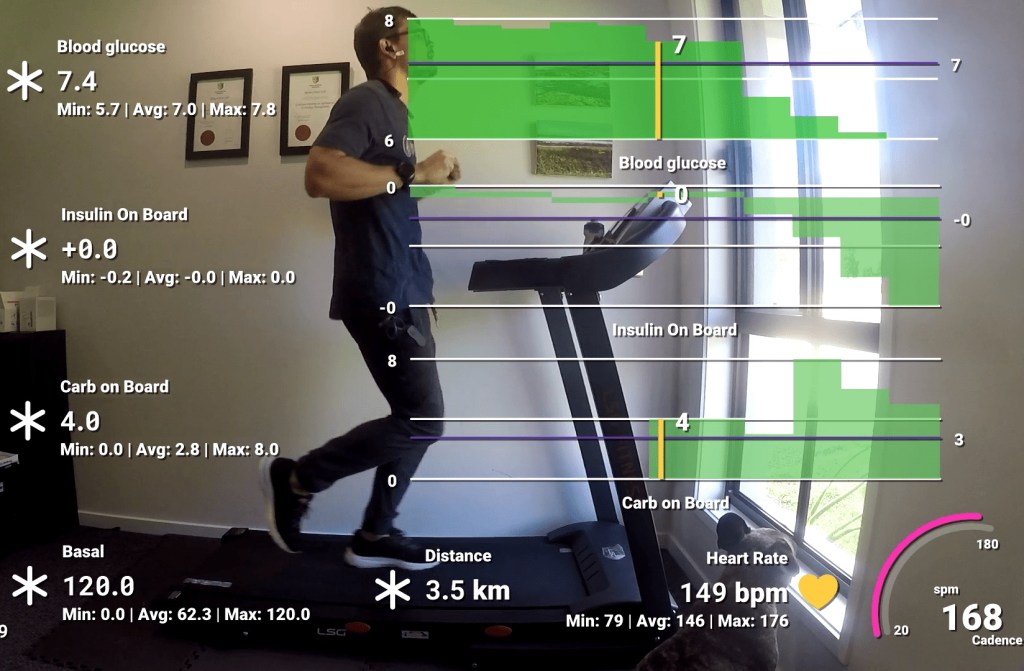
Video
I created a video using data from my Garmin Forerunner 245 and AAPS to track the experiment. In this video I track blood glucose, insulin, carbs, basal, distance, heart rate and cadence. I noted that the algorithm the Garmin uses to determine distance does not work well while walking and didn’t register any distance until I started lightly jogging.
In preparation for my cycle I started an automation to prepare my body for the impending exercise. This automation reduces my basal insulin ( as well as scale the rest of my management metrics) by 30% and set a temporary target (TT) of 7mmol/l. AAPS will not allow me to automate a profile % shift of more than 30%, so I reduced the profile a further 5% manually in AAPS an hour before the ride.
Exercise Metrics:
Garmin exercise stats
Blood Glucose:
Interestingly, AAPS stopped basal for a long period and allowed the IOB to runs its course.
My blood glucose held quite steady despite a mixture of anaerobic and aerobic levels of activity and so I didn’t need to consume any carbohydrates. Hopefully future attempts are as successful as this one.
It’s been 73 days since I started looping. I have had a difficult December with a sprained wrist from a mountain bike accident and myself, my daughter and my wife had gastro which resulted in very little sleep and some abnormal readings. In fact I am still having abnormal sensitivity to insulin, resulting in frequent lows or blood sugar swings. I also had two failed Dexcom sensors and moved to the code calibration method which resulted in two days of false high CGM readings in comparison to my blood glucose readings. I’ll add the CGM stats once I am finished the analysis. Hello 2022!
Blood Glucose Stats
Blood glucose stats
A marginal improvement in December over the fist two months, but I still have a lot of work to do to get to my goal of a 5.5% A1C. Interestingly enough, after the gastro I am now 40% more sensitive to insulin, so hopefully now that I am aware of this I can get back to better blood glucose readings. I will also need to run in open-loop when changing Dexcom sensors to avoid all the issues I was previously having with false high blood glucose readings causing my Loop to micro-bolus incorrectly or increase my basal in error. Still not sure how I will handle protein in open-loop.
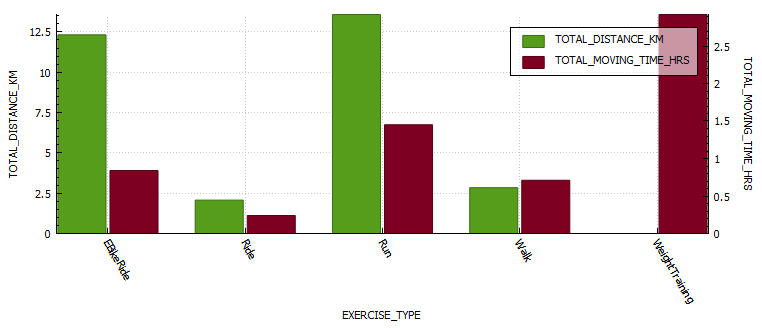
Exercise Stats 2021-2015
Total distance exercised
Total time spend exercising
I more than doubled (55%) the amount of hours I spent exercising in 2021, mostly as I was working from home which allowed me to spend more time exercising. As my A1C lowered, my fitness levels improved dramatically.
Disclaimer: The information contained within this blog post are my thoughts and do not constitute medical advice. Please consult your medical team before making any changes to your diet or program.
This guide is based on past experience, information obtained from other diabetics and input from a multitude of websites.
I have broken this guide up into 3 sections;
Pre-exercise (preparation)
Exercise
Post-exercise
Step 1: Pre-exercise
PUMP: BASAL: If you are on a pump, this usually involves setting a temp basal around an hour prior to exercise, but a multitude of factors will govern the % basal rate and how early you will start it. It seems a general rule of thumb is 30-70% depending on the intensity and duration of the exercise, the longer you exercise the more sensitive to insulin you will become. The faster (think Fiasp) your insulin responds to change, the shorter the waiting period prior to starting exercise could be. Short acting Insulin has a DIA (duration of insulin action) that usually lasts several hours (3-7ish), and any insulin you may have on-board (circulating within your body) will become more potent as you exercise, thus increasing the risk of a severe hypo.
MDI: BASAL: For most exercise under 40 minutes I would keep my basal the same and ensure I exercised in the morning, reducing the risk of a hypo by being fasted and by exercising during a period in time where we are more resistant to insulin. Of course you can exercise at any time you choose, but you need to be aware that if you did not adjust your basal according to your length and vigour of activity you are more likely to experience a hypo.
Snack and snack timing: If you exercise in the morning I prefer to exercise fasted provided the activity is under 40 minutes in duration. If the activity is over 40 minutes then I will have a small snack (under 15g of carbs) just before I set out. The carbohydrate requirements for individuals will differ according to your body composition (ie. smaller people require less fuel to achieve the same results as larger people would, or the more muscle you have the more fuel you will need). If I am exercising more than two hours after I woke up, I will require a snack to sustain me for the duration of the activity. I have found that 20-30 minutes after my snack seems to be my ideal time (snacks with higher protein / fat will digest more slowly than high carb snacks) to begin exercise. Its very much a process of monitoring and evaluating until you find what works for you.
Hypo treatments: Glucose, dextrose or sucrose in liquid form is by far the quickest and most precise way to treat an impending hypo. Its important to note that liquid is absorbed much faster than solid foods according to the Manhattan gastroenterology website. Ingesting solids foods during activity can result in post-exercise hyperglycaemia as the foods begin to digest soon after exercise stops.
“Exercise and digestion can be mutually exclusive. When you exercise, your body isn’t using its energy for digestion. Instead, it slows any digestion currently taking place so it can divert as much blood as it can to feed your muscles and your lungs.”
I use a Camelbak Podium bum bag to store my pump, glucose gels and Powerade.
Other items to consider:
Cannula placement; If the cannula is in the muscle group you plan to train, you may need to reduce basal further.
Sleep; If you are sleep deprived you may require more insulin.
Wake up period; If you are training within two hours of waking up, you may be more insulin resistant and require less pre-training fuel.
Pump suspension; If you suspended your pump you will need to consider the period of time that your pump is suspended as you will have missed that basal insulin.
Step 2: Exercise
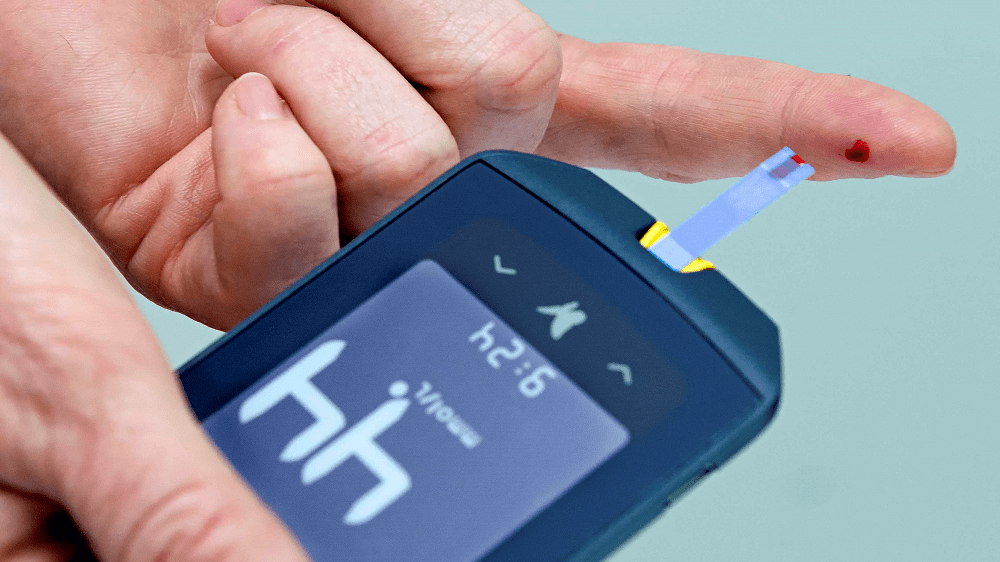
In my opinion, the most important things to do whilst exercising is to monitor and respond as required. I take my blood sugar at 15 minute internals when doing cardio ( I have a CGM attached to me at all times, but I prefer to use blood as its more accurate), which as you become more comfortable and attuned to your body, you could probably push to between 30 and 60 minutes to match testing to glycogen store depletion.
The average non-diabetic athlete has between 350-500g of stored glycogen when fully stocked (think high carb diets, the body stores less on lower carb diets) and up and 50% less glycogen just after waking up. These glycogen stores get fully depleted at around 90 minutes or 45 minutes if you exercise in the mornings . A Medivizor study suggested that diabetics have up to 21% less glycogen stores than the average person. If we consider the aforementioned statement regarding diabetics reduced capacity to store glycogen we realise that early morning exercise could lead to glycogen stores being depleted in as little as 35 minutes for the athletic individual, earlier if you are on a low carb diet or are untrained as your body uses glycogen less efficiently.
The Portland clinic advises that;
“During the first 15 minutes of exercise most of the sugar for fuel comes from either the blood stream or the muscle glycogen which is converted back to sugar. After 15 minutes of exercise, however, the fuel starts to come more from the glycogen stored in the liver. After 30 minutes of exercise, the body begins to get more of its energy from the free fatty acids”.
My personal experience seems to correlate to these findings and that’s why I test at 15 minute intervals, especially when starting a new routine, or restarting an old one. Also consider that you need insulin to utilise glycogen.
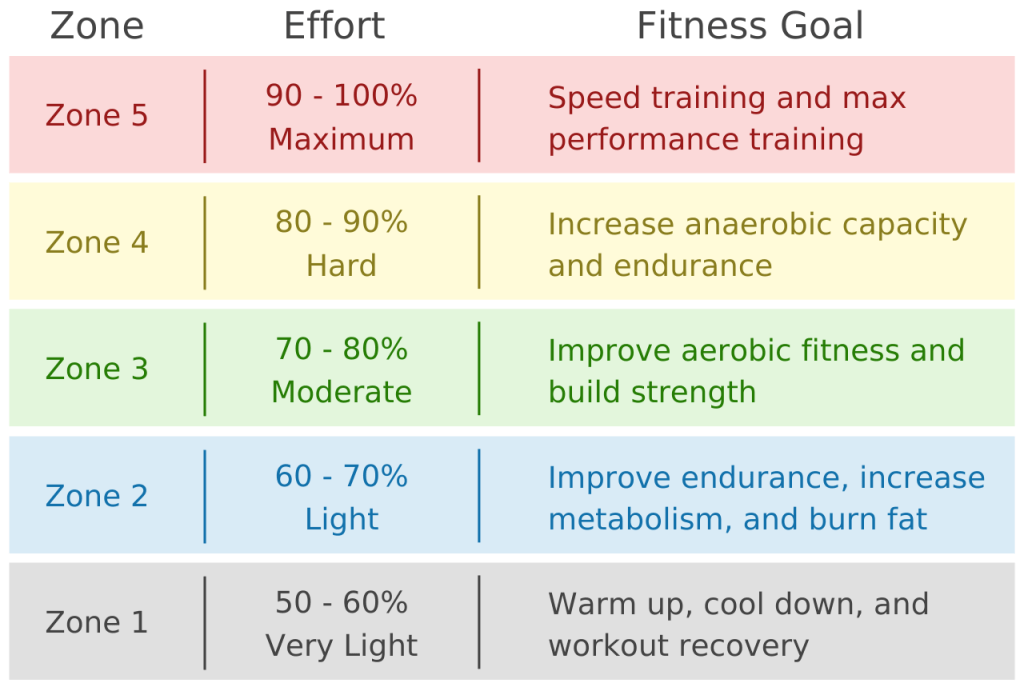
Effort levels can also influence blood glucose. Exercising at higher intensity levels can increase blood glucose due to stress hormones being released.
I use the formula 220-age to calculate my maximum heartrate. Then I can calculate effort from the below chart. I can then use this information to keep an eye on my heart rate during exercise and adjust my training effort as required. I also use this information to adjust my subsequent insulin doses as I am more sensitive to insulin an hour or two after exercise ( or directly post exercise when on MDI)
Starting Insulin recommendations in-line with activity durations
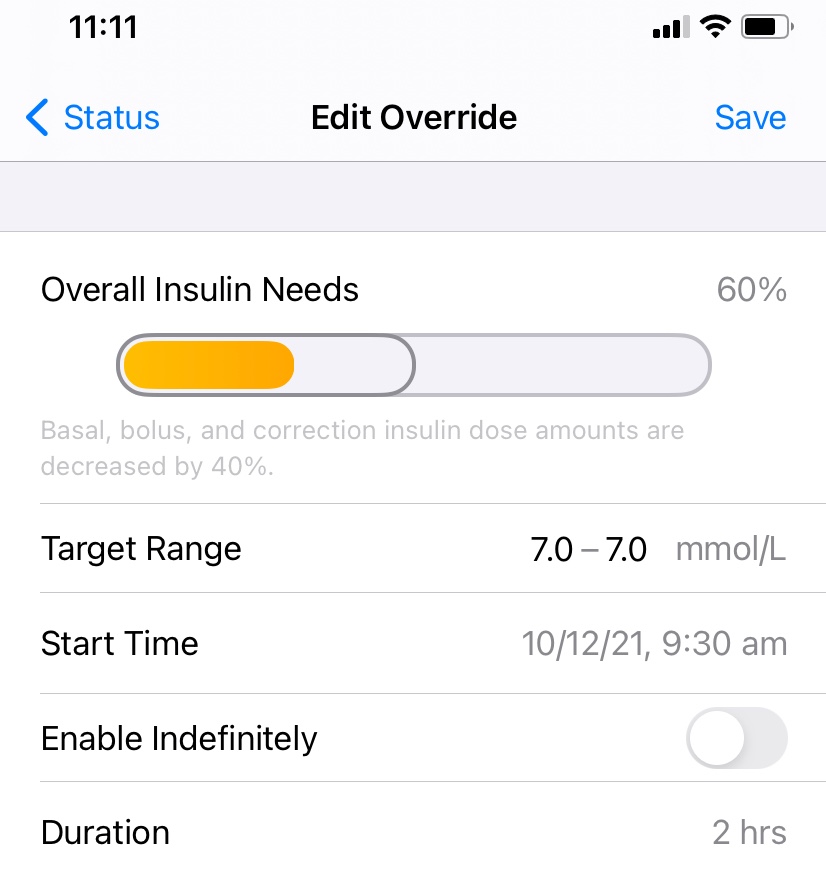
An example of how to use the table above would be if I had exercised at a moderate pace for 40 minutes, I could then experiment by decreasing my insulin dose by 67% and adjusting further if needed. Its easy to do this in Loop with temporary over-rides.
Temporary over-ride in Loop
An example of what I do to prepare for a run with Android Artificial Pancreas System (AAPS).
Step 3: Post Exercise
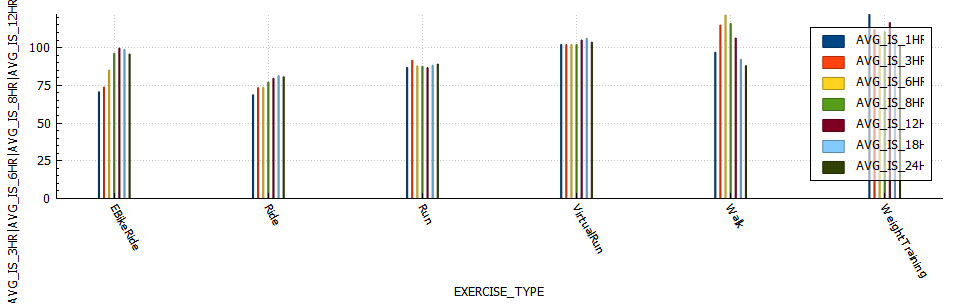
PUMP: I am not experiencing the sudden insulin sensitivity increase I did while on MDI. I believe this to be due to the fact that on MDI I cant reduce basal, but with the pump I can decrease basal as required. Be careful not to decrease your basal too much as your blood sugar will increase due to an inability to utilise glucose effectively. If you are using Loop then you could start a temporary over-ride to adjust insulin delivery for the remainder of the day. AAPS is capable of adjusting insulin requirements using a function called autosens which monitors deviations in insulin requirement. Below is a chart of insulin sensitivity post exercise grouped by exercise type.
MDI: I would generally be around 40% more sensitive to insulin immediately after a moderate run or cycle. This reason the onset of the sensitivity seems more rapid is due to the already circulating basal insulin now being super-charged. I found that exercising on MDI lacks some of the flexibility that pumps users have to adjust training duration or time period around your basal dose. On MDI I would the Spike app to adjust my meal time doses according according to the duration and intensity of the exercise. Spike is a very handy app for Apple MDI users to use as it can track meals, insulin and exercise. As well as have the functionality to calculate and adjust adjust insulin doses based on carbs and exercise input.
Screen capture of the the Spike-app.
NOTE: The Spike app is still available, it just requires a developer license and a significant time investment to install as its not available on test flight or the Apple store.
Today was a good day! After much trial and more research (through Facebook groups and medical literature) I finally figured out my recipe for staying in my range during cardio. It turns out I may have been too ambitious with my expectations of not eating before some heavy cardio.
The Process I followed was:
Set a temporary over-ride for my basal (40% reduction) and increase my target to 7.
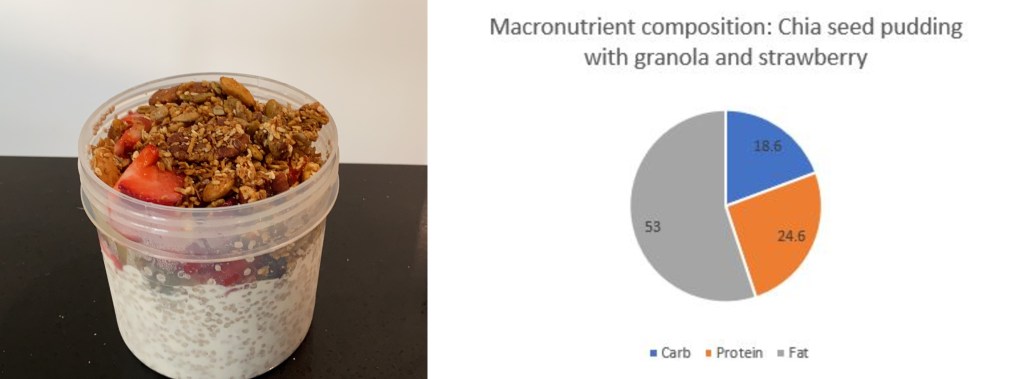
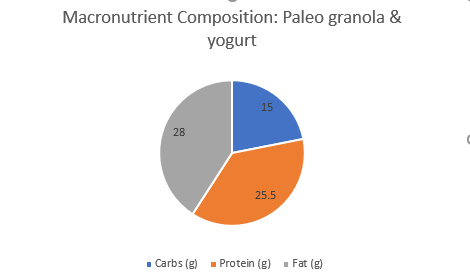
2. I ate a pre-run snack in the form of low carb granola and yogurt.
3. Waited for my glucose to rise above 6 ( I started at 6.8mmol/l)
4. Ran. I kept the loop closed as I wanted to see what would transpire. All in all I think it went well 🙂