Disclaimer: The information contained within this blog post are my thoughts and do not constitute medical advice. Please consult your medical team before making any changes to your diet or blood sugar management program.
So far 2022 has been quite the year. With the return to my work offices Its been rather difficult to reach many of the goals I set myself, but I did make progress. It seems 2023 is set to be a particular difficult year, but perhaps this will be the inspiration I need to make some positive changes. The Python scripts I wrote to export data from Nightscout to create my mountain bike videos seem to be working well and I can’t wait to make a few more videos.
I was curious to see if there were any differences in insulin sensitivity between longer and shorter activity durations, as well as higher intensity (where average heart rate was more than 80% of max heart rate) training and it seemed there was, it just wasn’t what I was expecting.
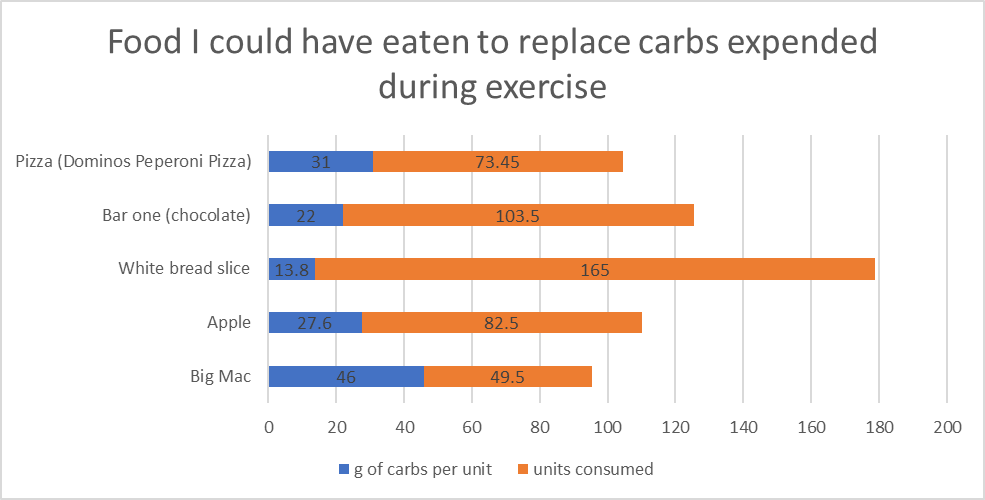
My average total daily dose (TDD) for 2022 was 32.9 units per day. If we analyse my aerobic activity (ride and runs) for the year and we use my sensitivity ratio from AAPS for 24 hours post exercise, I calculate that I saved 256 units of insulin in 2022 through exercise due to increased insulin sensitivity. During aerobic activity I consume 12g of carbs on average per 30 mins of activity unless I am exercising fasted. I can use this input to calculate that I ate 2277g of carbs during 2022. I would need 311 units of insulin to absorb 2277g of carbs. Since I don’t add carbs to AAPS while exercising I don’t have the exact numbers but I do believe this calculation to be pretty accurate. That equates to 49 Big Mac burgers / 82 Apples / 73 slices of Dominos peperoni pizza that I got to eat without insulin as a direct result of exercise.
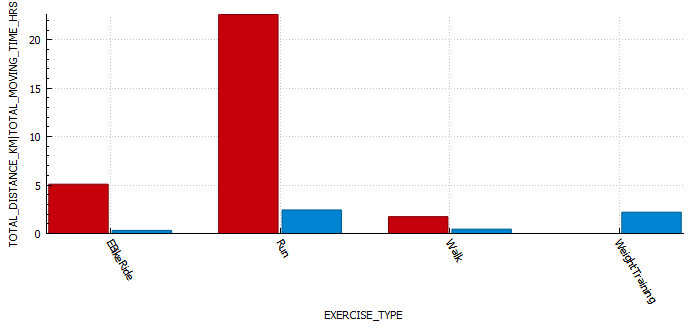
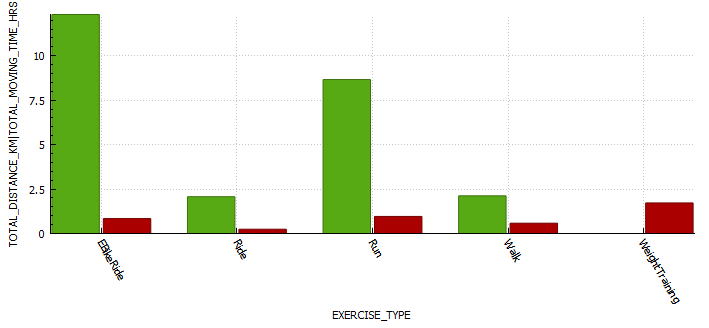
Exercise metrics
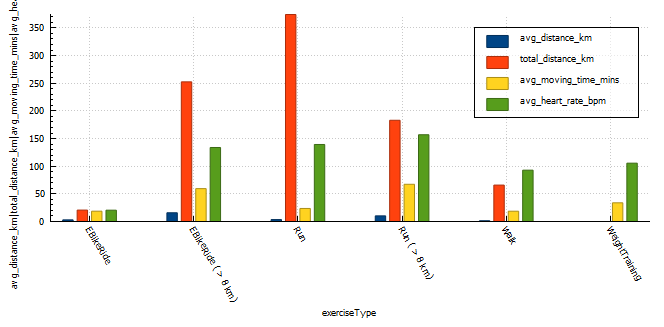
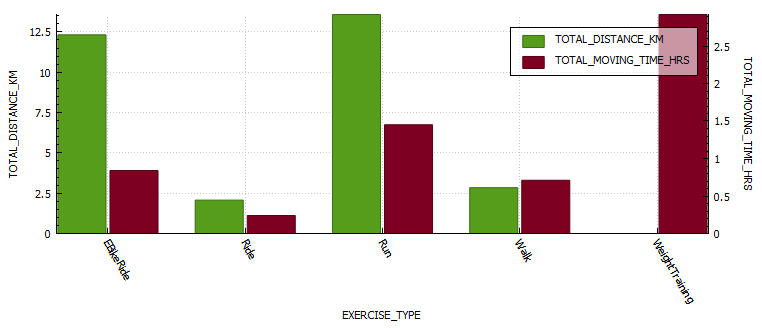
Analysing my exercise metrics I found that I was spending way too much time exercising at more than 75% of heart rate max, this would be hampering performance and building endurance. I did eighteen (18) runs at a distance greater than 8km, an improvement over the two (2) I did in 2021. I also managed my longest run ever at 16km.
exercise type
exercise count
total distance (km)
average distance (km)
average moving time (minutes)
average heart rate (bpm)
EBikeRide
7
20.64
2.95
18.65
N/A
EBikeRide ( > 8 km)
17
252.4
15.7
59.4
133.8 (72% max HR)
Run
108
374.25
3.47
23.5
139.26 (75% max HR)
Run ( > 8 km)
18
183.1
10.1
67
156 (85% max HR)
Walk
48
65.8
1.37
18.6
93 (50% max HR)
WeightTraining
65
0.0
0
33.77
105 (57% max HR)
TOTAL
262
896
5.6
36
125 (68% max HR)
Exercise stats table for 2022
Time-in-range (TIR)
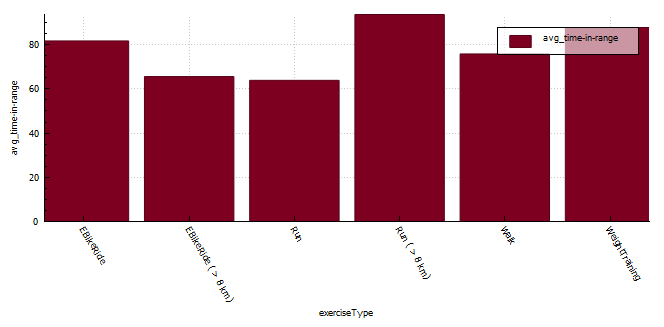
The longer distance running seem to result in the best time-in-range (TIR) (3.9-7.8 mmol/l) but I do feel that these runs also seem to happen at a similar time in the morning where I have more control over insulin-on-board (IOB) and carbs-on-board (COB) and I am the most resistant to insulin. My heart rate is also far more consistent (aerobic) during running than when mountain biking ( aerobic / anaerobic ).
If I start digging into the data for short runs more closely I find that;
TIR (3.9-7.8 mmol/l) from 04:00am – 10:00am is 63%
TIR (3.9-7.8 mmol/l) from 10:00am – 13:00pm is 83%
TIR (3.9-7.8 mmol/l) after 13:00pm is only 23%
exercise type
exercise count
time-in-range (%)
EBikeRide
7
81.67
EBikeRide ( > 8 km)
16
65.56
Run
108
56.8
Run (04:00 – 10:00 am)
18
63.8
Run (10:00 – 13:00 pm)
61
83.6
Run (13:00 – 10:00pm)
29
23.02
Run ( > 8 km)
18
93.6
Walk
45
75.8
WeightTraining
65
87.7
Exercise time-in-range table for 2022
Blood glucose control metrics
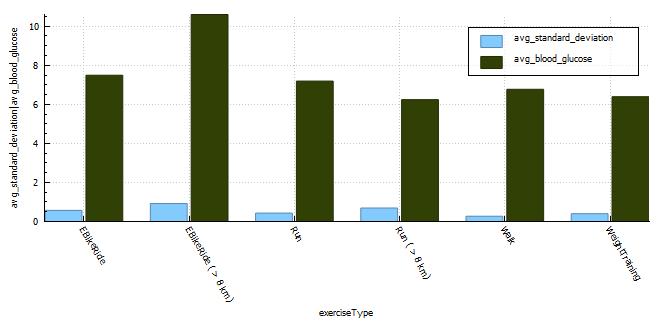
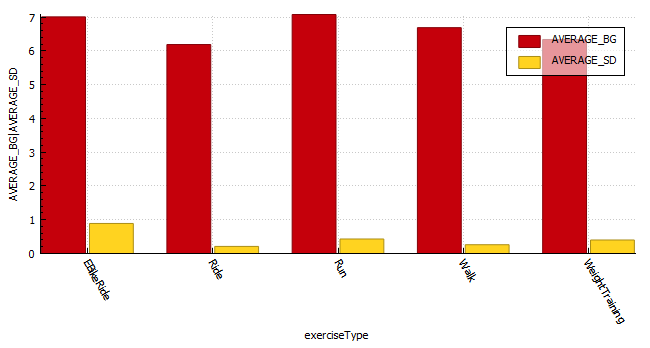
The exercise that resulted in the lowest blood glucose fluctuations is walking with a CV of 4%. The exercise with the second lowest CS was weight training. I generally try to train with a little insulin-on-board to counteract the hormones released during training and I don’t need to set a high temp target in the lead-up to the activity, thus my reading is much lower at exercise commencement. The third lowest is short runs (< 8km) with CV of 6%. The higher blood glucose average will be a direct result of me setting a higher temp target (8 mmol/l) prior to exercising, but the duration of activity isn’t long enough to reduce the blood glucose substantially resulting in the high average. Long runs seem to result in the least stable blood glucose values with a CV of 12% but the average for long runs is lower as the sustained activity reduces blood glucose. I suppose on these longer runs I do consume a minimum of 30g of ultra-fast acting carbs (glucose, dextrose) which is going to result in some fluctuations in blood glucose.
With coefficient of the variation (CV) a lower percentage is indicative of more stable blood glucose readings.
exercise type
exercise count
average standard deviation
average blood glucose
average coefficient of the variation (CV)
EBikeRide
7
0.57
7.49
8%
EBikeRide ( > 8 km)
16
0.92
10.6
9%
Run
108
0.43
7.19
6%
Run ( > 8 km)
18
0.69
6.24
11%
Walk
48
0.27
6.77
4%
WeightTraining
65
0.4
6.39
6%
Exercise breakdown for 2022
Insulin sensitivity
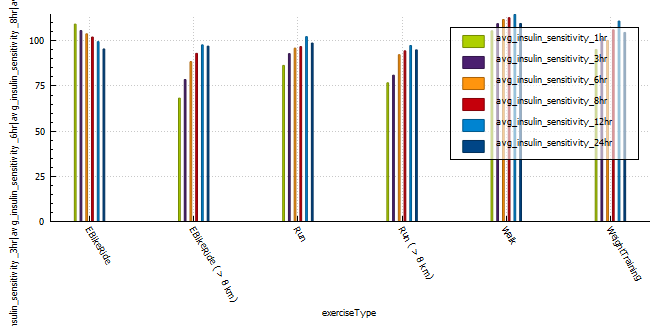
A very interesting observation was that longer, more intense activity resulted in sensitivity returning to normal quicker than less intense or shorter activity. Runs shorter than 8km resulted in a massive 12% insulin reduction for 24 hours post activity, that’s around 6.5 units less insulin in a 24 hour period. Long E-Bike rides resulted in the largest increase (35%) in sensitivity 1 hour post activity, with shorter E-Bike rides the second largest increase in sensitivity. Runs longer than 8 km increased sensitivity (25%) the third most, but the body seemed to return to normal more quickly than the shorter runs and was almost back to normal within 12 hours of activity.
(NOTE: I can’t comment on the validity of the results, only that patterns exist after exercise that are not usually observed in the absence of aforementioned exercise.)
average insulin sensitivity
exercise type
exercise count
1 hr post exercise
3 hr post exercise
6 hr post exercise
8 hr post exercise
12 hr post exercise
24 hr post exercise
EBikeRide
7
109
105
103
102
99
95
EBikeRide ( > 8 km)
16
68
78
88
93
97
79
Run
108
86
92
95
96
102
98
Run ( > 8 km)
18
76
80
92
94
97
94
Walk
48
105
109
111
112
114
109
WeightTraining
65
95
101
100
106
110
104
Average insulin sensitivity for multiple time blocks post exercise grouped by exercise type.
Profile Adjustments vs. Temporary Targets (TT)
In the past I used a combination of a 30% reduction in profile and a temporary target of 7 mmol/l while exercising.
This seemed to work quite well, with the caveat that profile adjustments can result in your autosens data being reset if you cancel the adjustment earlier than set.
One way to combat this is to set a higher temp target, this will not effect sensitivity data and can be cancelled at any time without needing to update the basal insulin profile in the pump of effecting autosense data. In order to do this I analysed the adjustments I was using to calculate a temp target that should reduce my insulin enough to keep me in range for the duration of activity.
It’s diabetes awareness month and so I wanted to talk to you about something I am very passionate about, Android artificial pancreas system (AAPS). It’s not the cure I wanted but as far as I am concerned, it’s the closest to normal I have felt in the 25 years I have been a diabetic.
Why ILOVEAndroid APS
I decided to try Android APS just prior to the birth of my daughter. At the time I was using multiple daily injections (MDI) on a low-carb diet (less than 45g per day excluding protein and fat) and trying to pick up some muscle. I found it rather challenging to eat the number of carbs the trainer suggested without compromising control. I was also anticipating the late nights having a baby entails and I wanted to be prepared. David Burren’s blog provided a blueprint of what could be expected if I committed to investing the time required to perform all necessary testing and fine-tuning.
Benefits of Android APS
Meal management
Meals can be managed through a number of mechanisms including;
Un-announced meals (UAM) – AAPS boluses insulin without intervention or carb entry.
Announcing carbs – Add the carbs into the system and the calculator estimates the amount of insulin required based on your COB, IOB, ISF, current blood glucose, blood glucose deltas, and insulin sensitivity.
Extended carbs – typically used to mimic the absorption of protein (gluconeogenesis) or delayed gastric emptying caused by high-fat meals.
Exercise management
Insulin scaling adjusts basal insulin based on current insulin sensitivity
Automations allow you to schedule profile changes and temporary blood sugar targets for the duration of activity or condition.
Directly or indirectly (via Nightscout) display various blood glucose-related data on compatible watches. If you are using an Android watch (WearOS) you can control AAPS via the watch. Garmin watches can display blood glucose data during an activity.
Utilise the blood glucose data from a wide variety of CGMs (continuous glucose monitors)
Software
Automations allow you to automate system actions based on conditions (eg. blood glucose increasing, blood glucose decreasing, leaving for work, pump disconnect) or schedules.
Highly customizable to your unique needs, with certain advanced builds allowing you to control more system variables (Boost, AIMI, Eating Now).
Cutting-edge development
Dynamic insulin sensitivity factor (ISF that changes based on blood glucose)
Improved prediction models
Improved insulin modeling (9-hour DIA)
Quality of Life
Reduced diabetic burden and stress.
Glucose is constantly monitored, with the ability for someone to follow you remotely, including community members. This can assist with fine-tuning settings.
Ability to eat more foods without compromising control
Improved glucose control reduces the possibility of long-term complications.
Safety
Objectives provide a level of safety as users need to understand basic principles of how to use the APS prior to closing the loop.
Nightscout reporter provides detailed reports that can assist with APS tuning and a detailed view of your risk rate through the comprehensive glucose pentagon.
As with all DIY systems, you are required to build the application prior to using it.
Cost of hardware
Phone
CGM
Pump and supplies
Connectivity fatigue
The burden of being connected to technology 24/7
Reliance
It is easy to become reliant on AAPS managing blood sugars.
Usability
Due to its complexity, you are required to invest a large amount of time in order to gain the understanding and skills required to configure and utilise it correctly.
Statistics and examples:
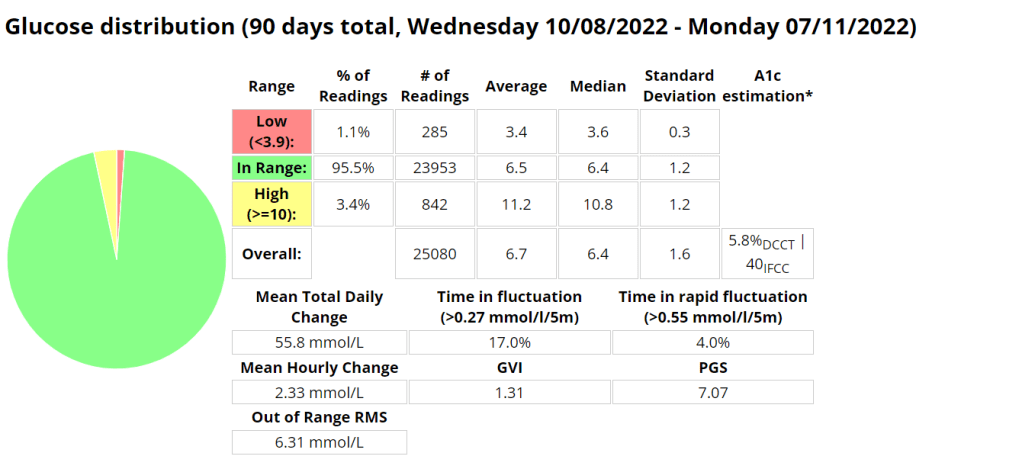
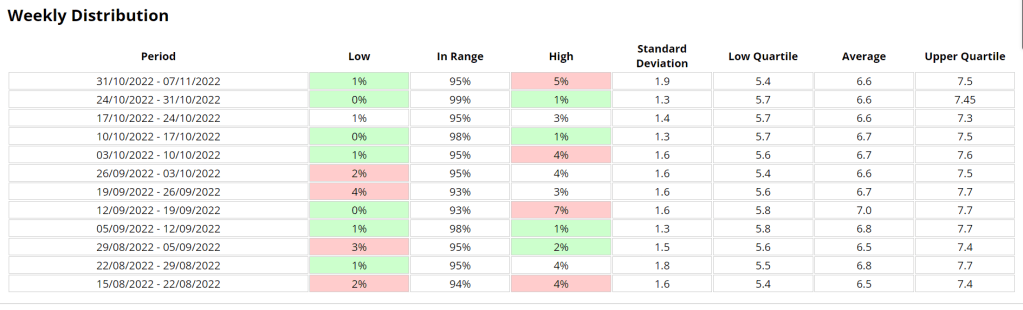
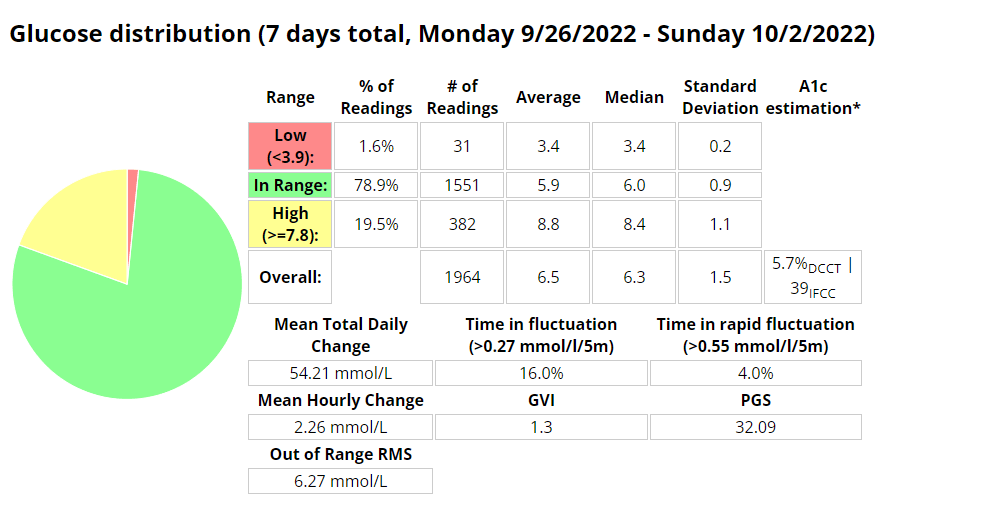
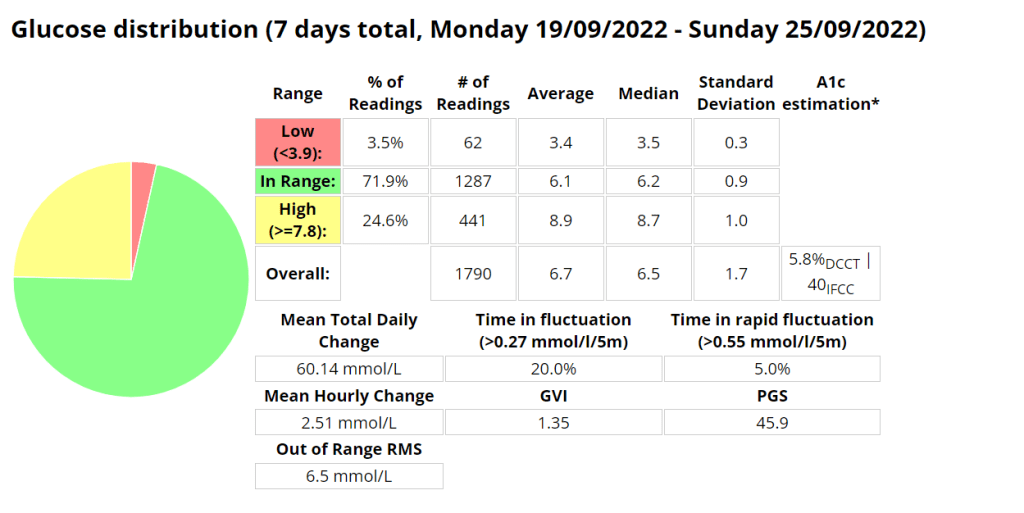
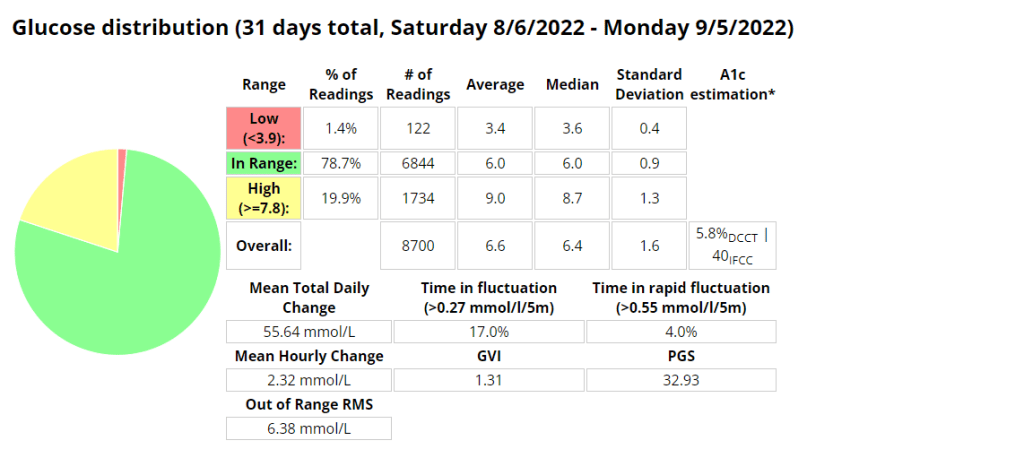
Nightscout statistics – 3 Months
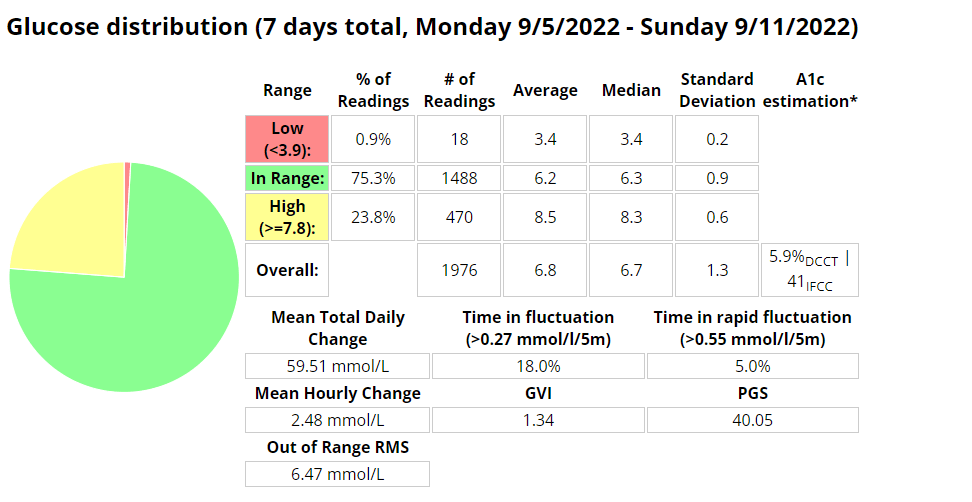
Nightscout blood glucose distribution reportNightscout blood glucose weekly distribution report
Control stats for different systems
Date Started Test
Control Mechanism
e-A1C
Average Blood Glucose
Time In Range (TIR) 3.9 – 10
Standard Deviation
Average carbs consumed
GVI
PGS
CGP – PGR
20/11/2019
MDI
6.1%
7 mmol/l
87%
2.2 mmol/l
1.2
20.33
1.7
20/11/2020
MDI
5.6%
6.3 mmol/l
94%
1.7 mmol/l
< 60
1.17
8.67
1.3
20/11/2021
Loop
5.7%
6.5 mmol/l
94%
1.7 mmol/l
<100 (carb counting)
1.25
8.29
1.3
04/02/2022
Android APS
5.7%
6.5 mmol/l
96%
1.5 mmol/l
>200, little to no carb counting
1.24
5.70
1.2
Analysis stats provided by Nightscout reporter.
Comprehensive glucose pentagon from Nightscout reporter report.
Un-announced meal (UAM) example
Low-carb meal with UAM running (Low-carb bread with cheese, ham, and mayo.)
Extract from Android APS data for a low carb meal
As can be seen above the system manages low-carb meals quite well with no carb inputs from the user. The system constantly monitors for rapid changes in blood sugars and administers insulin when required to quickly brings sugars into range.
Nightscout screenshot of low carb meal being absorbed while AAPS manages sugars.
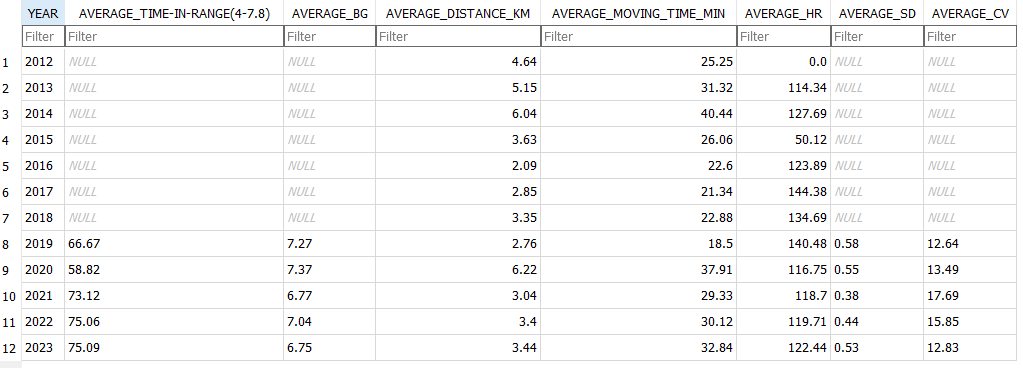
Exercise stats / examples
Year
Average Time in Range (3.9-7.8 mmol/l)
Average blood glucose (mmol/l)
Average Standard Deviation (mmol/l)
Total Hours
Total KM
2022
80.1 %
6.6
0.43
131
885
2021
71.9 %
6.7
0.4
149
920
2020
69.7 %
6.9
0.7
67
658
Annual improvements are made through tweaking system variables and my approach to exercise.
Weight Training
Date
IOB @ start
Moving time
Exercise Type
Average HR (bpm)
Standard Deviation (mmol/l)
CGM BG Start
CGM BG End
CGM BG Average (mmol/l)
TIR (3.9-10)
2022-10-07
0.14
36.93
WeightTraining
101.1
0.365
7.7
6.8
7.27
100.0%
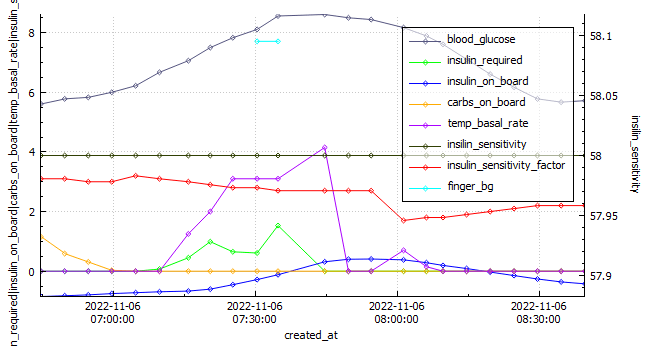
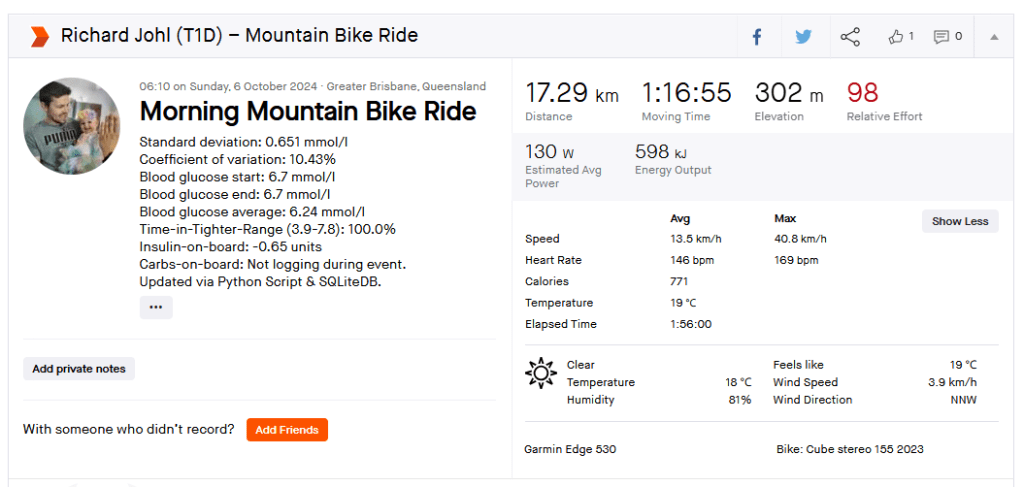
EBike Ride
Android APS data exported during an E-Bike Ride 2022-11-06.
Date
IOB @ start
Moving time
Exercise Type
Distance (km)
Average HR (bpm)
Standard Deviation (mmol\l)
CGM BG Start
CGM BG End
CGM BG Average (mmol\)
TIR (3.9-10)
2022-11-06
-0.849
115.92
eBikeRide
27
143
1.095
5.9
5.8
7.16
100%
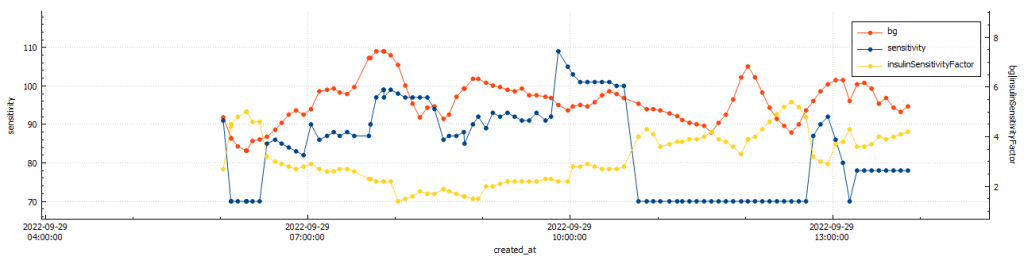
Running
Android APS data exported during a run 2022-10-03.
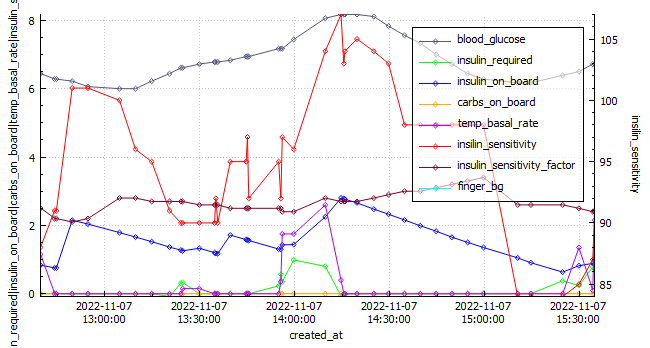
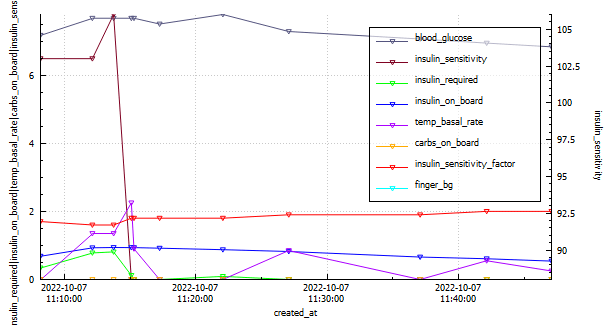
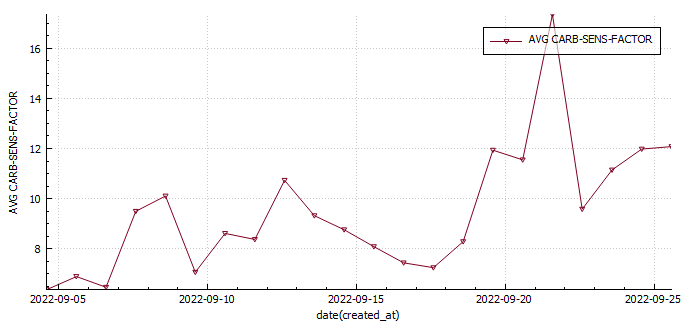
This week was the best so far. I did my longest run to date (12km) and had a really good gym week lifting (approx. 20% more volume). My diabetes control is improving (thank you AAPS and exercise) and I have learned a lot digging though my data and through responses from the previous weeks question regarding carb sensitivity factor (CSF) being used to measure insulin sensitivity post exercise. I made some strides in my glucose management tool which also felt great.
BG vs. ISF vs. insulin sensitivity post gym (@11:48:09 – 42min)BG vs. ISF vs. insulin sensitivity post run (@11:49:30 – 33min)
After gym sensitivity increased to 115% directly post training, while my sensitivity was stable at 78% post my run.
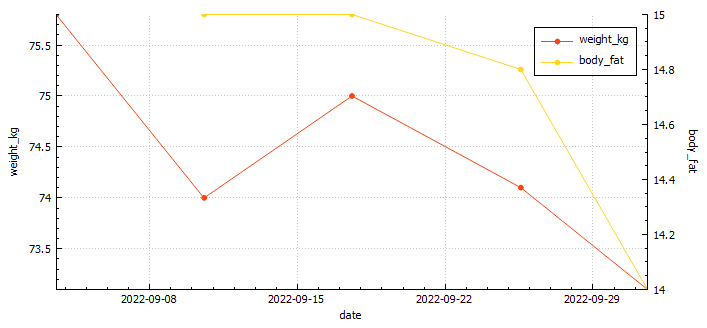
Body Metrics
Body mass vs. body fat
Start
Week 1
Week 2
Week 3
Week 4
Weight (kilograms)
75.8
74
75
74.1
73.1
Body fat percentage (according to Samsung)
17.3%
17.8
*
*
Body fat percentage (according to the navy seal calculator)
15%
15%
14.8%
14%
Total volume
Table stating the weekly body metrics I am tracking.
Exercise
Week 1
Week 2
Week 3
Week 4
Distance (kilometres)
25.17
20.54
37.22
29.4
Activity (hours)
4.34
3.65
5.64
5.4
Table stating the weekly exercise metrics I am tracking
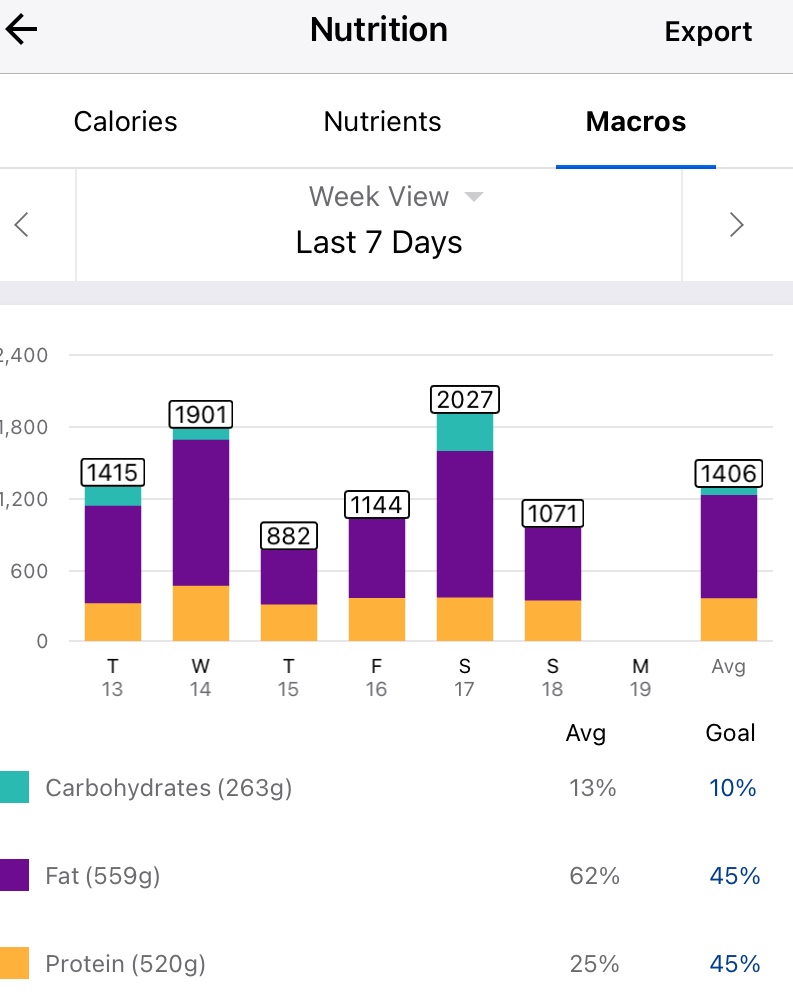
Nutrition
Screenshot of average macro-nutrients consumed during week 4
Screenshot of average macro-nutrients consumed during week 4
Diabetes
Week 1
Week 2
Week 3
Week 4
Low (<3.9) (%)
0.9
0.6
3.5
1.6
In Range (3.9-7.8) (%)
75.3
74.7
71.9
78.9
High (>= 7.8) (%)
23.8
24.7
24.6
19.5
Standard deviation (SD)
1.3
1.7
1.7
1.5
Average (mmol/l)
6.8
7.0
6.7
6.5
A1c estimation (%)
5.9
6.0
5.8
5.7
Table stating the weekly diabetic metrics I am tracking.
Ideally I want to see a time-in-range (TIR – 3.9-7.8 mmol/l) exceeding 90% with an average in the low sixes and a standard deviation (SD) around one (1).
I am starting to feel like a routine is forming, perhaps not around diet yet, but definitely in regards to training. In previous years of doing this I was eating clean most days, as it provided improved diabetic control in the absence of an APS/AID and pump.
This week was particularly heavy due to my birthday dinner, a new phone, a new version of AAPS (Boost test platform 3.6.5) and a 25 km cycle. *I have been unable to pair my galaxy watch with my new phone, which is sad as I really liked the watch and having the plethora of sensors.
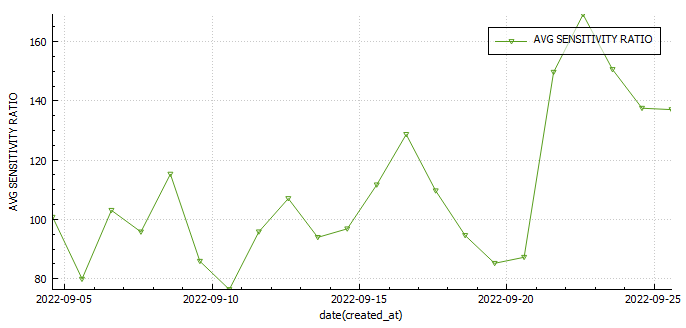
I was investigating the possibility of measuring insulin sensitivity changes in AAPS . One way would be to use the autosens feature in AAPS , but since I wasn’t including the carbs I ate to fix hypos, and I was snacking in-between to keep my readings steady that wasn’t going to work. The only metric that may prove useful may be my carb sensitivity factor (CSF). The average CSF over the 22 days so far is 8.7 while the average sensitivity ratio was 106%. This would mean that according to CSF I was 36% more sensitive to carbs yesterday or 29% less sensitive according to autosens.
Body Metrics
Start
Week 1
Week 2
Week 3
Week 4
Weight (kilograms)
75.8
74
75
74.1
Body fat percentage (according to Samsung)
17.3%
17.8
*
Body fat percentage (according to the navy seal calculator)
15%
15%
14.8%
Total volume
Table stating the weekly body metrics I am tracking.
Exercise
Week 1
Week 2
Week 3
Week 4
Distance (kilometres)
25.17
20.54
37.22
Activity (hours)
4.34
3.65
5.64
Table stating the weekly exercise metrics I am tracking
Nutrition
Screenshot of average macro-nutrients consumed during week 3
Screenshot of average macro-nutrients consumed during week 3
Diabetes
Week 1
Week 2
Week 3
Week 4
Low (<3.9) (%)
0.9
0.6
3.5
In Range (3.9-7.8) (%)
75.3
74.7
71.9
High (>= 7.8) (%)
23.8
24.7
24.6
Standard deviation (SD)
1.3
1.7
1.7
Average (mmol/l)
6.8
7.0
6.7
A1c estimation (%)
5.9
6.0
5.8
Table stating the weekly diabetic metrics I am tracking.
Ideally I want to see a time-in-range (TIR – 3.9-7.8 mmol/l) exceeding 90% with an average in the low sixes and a standard deviation (SD) around one (1).
The second week I have gained a little weight (surprise its not muscle) and had a reduction in exercise hours, which was mostly due to a very long ride I had the previous week.
My diabetic metrics have declined and I feel like all of this mostly due to my diet which needs tweaking.
Body Metrics
Start
Week 1
Week 2
Week 3
Week 4
Weight (kilograms)
75.8
74
75
Body fat percentage (according to Samsung)
17.3%
17.8
Body fat percentage (according to the navy seal calculator)
15%
15%
Total volume
Table stating the weekly body metrics I am tracking.
Exercise
Week 1
Week 2
Week 3
Week 4
Distance (kilometres)
25.17
20.54
Activity (hours)
4.34
3.65
Table stating the weekly exercise metrics I am tracking
Nutrition
Screenshot of average macronutrient consumed during week 2
Screenshot of average macronutrient consumed during week 2
Diabetes
Week 1
Week 2
Week 3
Week 4
Low (<3.9)
0.9%
0.6%
In Range (3.9-7.8)
75.3%
74.7%
High (>= 7.8)
23.8%
24.7%
Standard deviation (SD)
1.3
1.7
Average
6.8
7.0
A1c estimation
5.9%
6.0%
Table stating the weekly diabetic metrics I am tracking.
Ideally I want to see a time-in-range (TIR – 3.9-7.8 mmol/l) exceeding 90% with an average in the low sixes and a standard deviation (SD) around one (1).
Before my run yesterday my blood glucose was lower than I felt was safe to start exercising (around 4 mmol/l ) despite reducing insulin to 70% of requirements and setting a higher temp target ( 7 mmol/l) an hour prior to exercising. I decided to eat an Anzac cookie (20g carbs) and accidently devoured some deep fried bread (30g of carbs). This was excessive to say the least ( I needed around 12g according to my calculator). It also created a complicated situation where I would need to inject prior to exercise or forego exercising all together and rather focus on injecting the appropriate amount of insulin (8.62 units) to counteract the carbs.
Factors to consider
As a rule of thumb I try to have as little insulin on-board as possible as this reduces the chances of hypoglycaemia (low blood sugar). Due to the carbs I ate I would now need to inject insulin prior to exercising or my blood glucose would rise excessively. I factored in that both fat (from the fried bread) and exercise would decrease the speed of digestion. Exercise decreases the speed of digestion as energy used for digestion would be diverted to my heart, lungs and muscles to fuel my activity and fat slows down gastric emptying and causes insulin resistance.
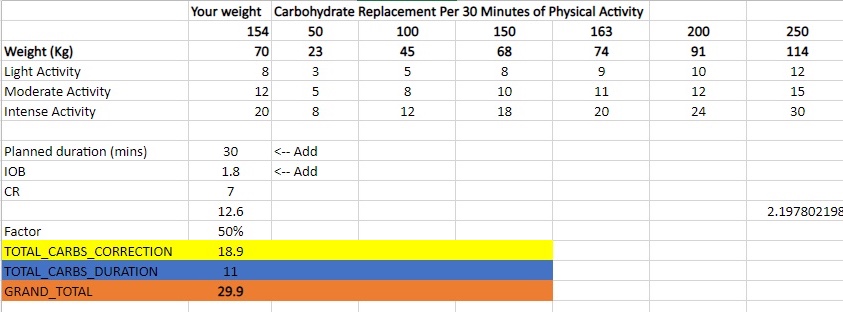
Insulin calculation
Utilising my IC ratio and exercise table I calculated I required around 1.7 units of insulin prior to the commencement of my run. I decided to be cautious and inject 1.5 units. I used a total of 4.4 units to return to euglycemia (normal blood sugar).
Insulin-to-carb ratio
carbs
Insulin Required
75%
50%
25%
20%
15%
5.8
50
8.62
6.47
4.31
2.16
1.72
1.29
Insulin calculation table
Table containing the amount of carbs I require for a specific duration of activity. This was derived from information found on the internet and my own experience.
Results
The results were by no means perfect, but at the very least I learned how much insulin I require and more or less when I should be injecting after I finish exercising. Its extremely difficult to predict how much exercise will amplify insulins activity, so it’s always safer to take a cautious approach.
My final decision was to inject 1.5 units prior to starting my activity and inject the remaining amount once my sugars started rising due to digestion resuming (around 35 minutes after stopping exercise).
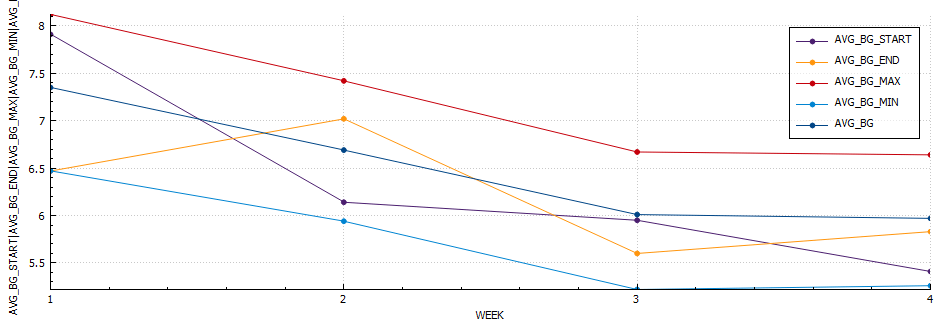
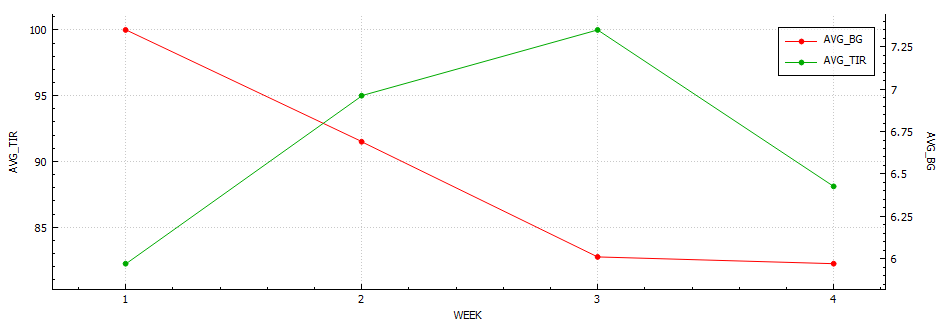
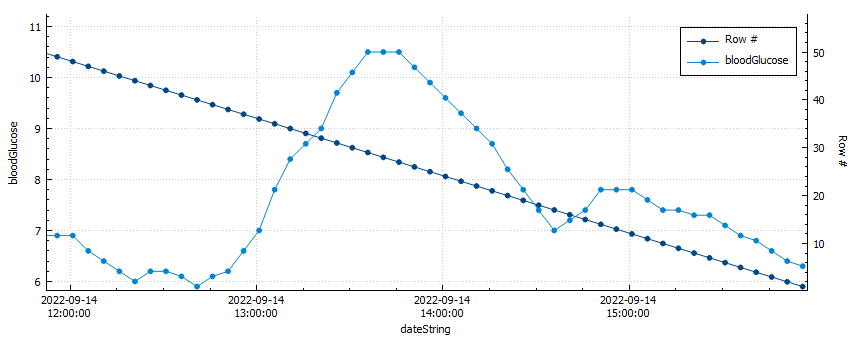
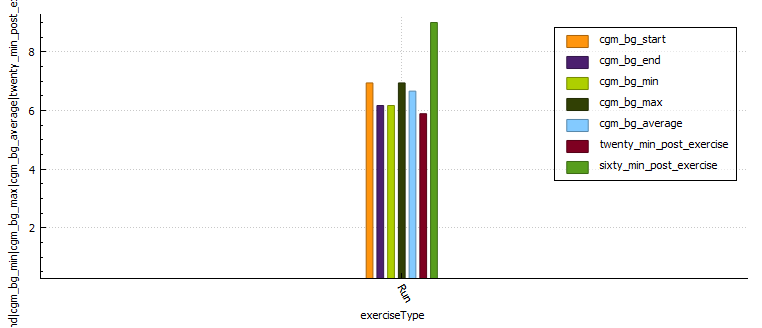
Blood glucose vs. row count
My blood sugar peaked at 10.5 mmol/l after only 1.5 units of insulin for 50g of carbs.
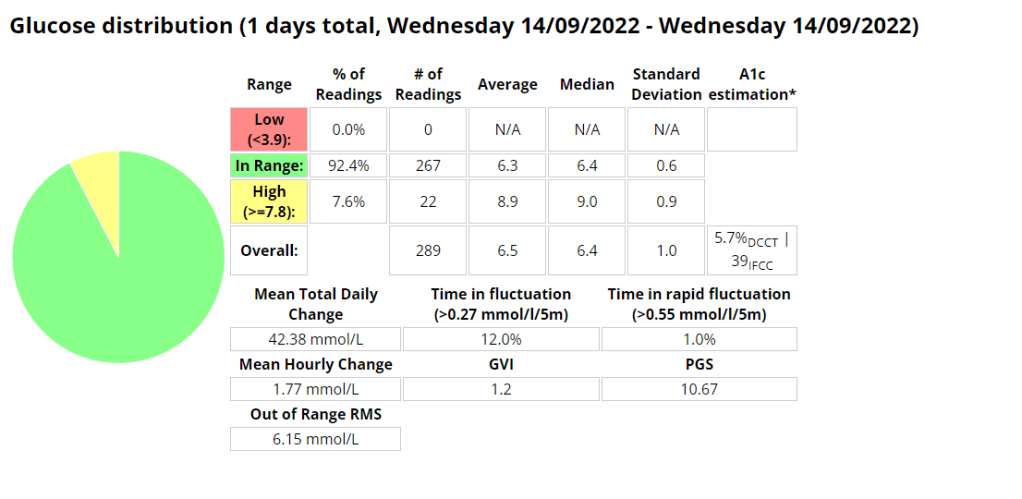
I used a total of 4.4 units of insulin (50% of the total insulin required) to return to euglycemia after my activity. My average blood glucose was 6.6 mmol/l and my time-in-range (TIR) was 100% for the duration of my activity.
Graph with glucose control metrics during activity
Distance (km)
Moving time (minutes)
Average heart rate
Standard deviation
CGM BG start
CGM BG end
CGM BG min
CGM BG max
CGM BG average
Time in range
BG twenty minutes post exercise
BG sixty minutes post exercise
Lunch Run
4.92
29.53
170.2
0.308
6.94
6.17
6.17
6.94
6.66
100.0
5.89
9.0
Glucose control metrics
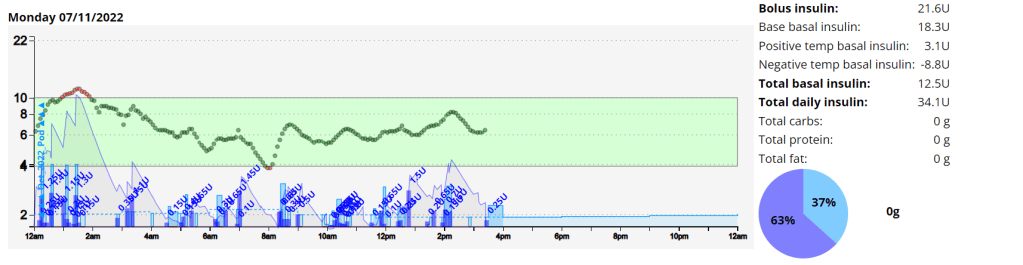
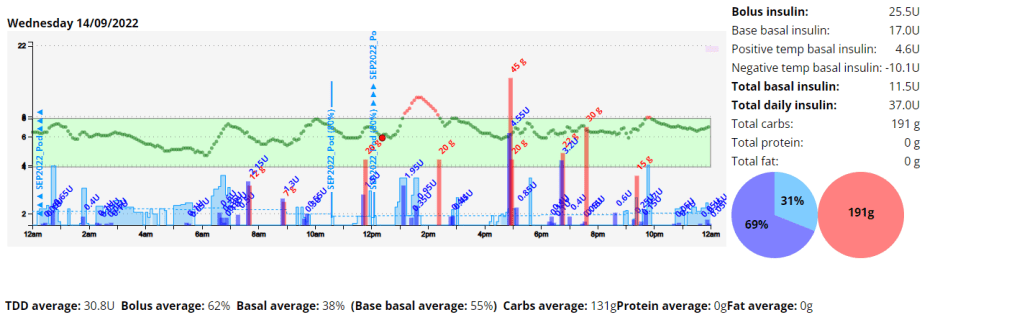
Daily overview graph with insulin and carbs.Diabetic management metrics.
My blood sugar control after exercise improved and I was happy with the results for the remainder of the day. Next time I would inject 20 minutes post exercise to prevent digestion resuming causing hyperglycaemia (high blood glucose).
The first week was challenging to say the least. As I have increased my physical activity my insulin needs seem to have fundamentally changed, and this resulted in quite a few lows. I also had some tech issues, my Android phone had an operating system error and my Dexcom sensor wasn’t enjoying the resistance training I was doing as it was inserted in my arm. I reached my activity goals but exceeded my diabetic and nutritional goals.
Body Metrics
Start
Week 1
Week 2
Week 3
Week 4
Weight (kilograms)
75.8
74
Body fat percentage (according to Samsung)
17.3%
Body fat percentage (according to the navy seal calculator)
15%
Total volume
Table stating the weekly body metrics I am tracking.
Exercise
Week 1
Week 2
Week 3
Week 4
Distance (kilometres)
25.17
Activity (hours)
6.24
Table stating the weekly exercise metrics I am tracking
Week 1 breakdown
Nutrition
Screenshot of the average and total macronutrients consumed during week 1.
Screenshot of average macronutrient consumed during week 1
Diabetes
Ideally I want to see a time-in-range (TIR – 3.9-7.8 mmol/l) exceeding 90% with an average in the low sixes and a standard deviation (SD) around one (1).
Two years ago my daughter was born. At this time I was off work for a few weeks and I had been strongly considering writing a tool that could provide some insight into managing my blood sugars, as I knew controlling my blood sugar was the best chance I had of being the best parent I cold be. At the time I was on multiple daily injections (MDI), leveraging heavily on Dr Bernstein’s teachings and using daily (if possible) exercise as a tools for glucose control.
Two years later the tool has pivoted many times, and at one time I was using machine learning (ML) to predict blood glucose during exercise, until I started using the Dexcom G6 continues glucose monitor (CGM) which was accurate enough to circumvented the need for the aforementioned tool.
At present I am using an automated insulin delivery (AID) device to deliver most of my insulin based on my shifting needs. This significantly reduces the mental burden required for good glycaemic control, as well as reduce some of the anxiety I was experiencing at meals times and when going to the doctor for diabetic checks. This system still requires manual input prior to exercise and constant tuning if you want to have the best experience, and so my tool has pivoted towards analysing this data and providing insight there.
Diabetic Metrics
An analysis of the last 4 years of my diabetic journey highlights a better A1C with a lower standard deviation (SD) indicating more consistency in blood sugars. Its interesting to note the much improved time-in-range (TIR-IN) metrics once I moved over to a insulin pump using an automated insulin delivery (AID) device.
Period
Hypo (below 3.9)
In (3.9-10)
High (above 10)
Average
A1C
SD
GVI
PGS
PGR
PGR-Risk
Exercise hours
Kilometres
Pump / MDI
2019
19%
77%
3%
7.7
6.50%
2.6
1.26
40.19
2.2
Low
16
146
MDI
2020
8%
88%
3%
6.9
6.00%
2.1
1.19
17.34
1.6
very-low
67
658
MDI
2021
3%
94%
3%
6.4
5.60%
1.7
1.18
8.79
1.3
very-low
149
920
Pump (Loop) 20/11/2021
2022 (YTD)
3%
96%
1%
6.5
5.70%
1.5
1.2
5.43
1.2
very-low
75
496
Pump (AAPS)
Table displaying the last few years worth of diabetic data.
For a description of some of these values mean please read this article.
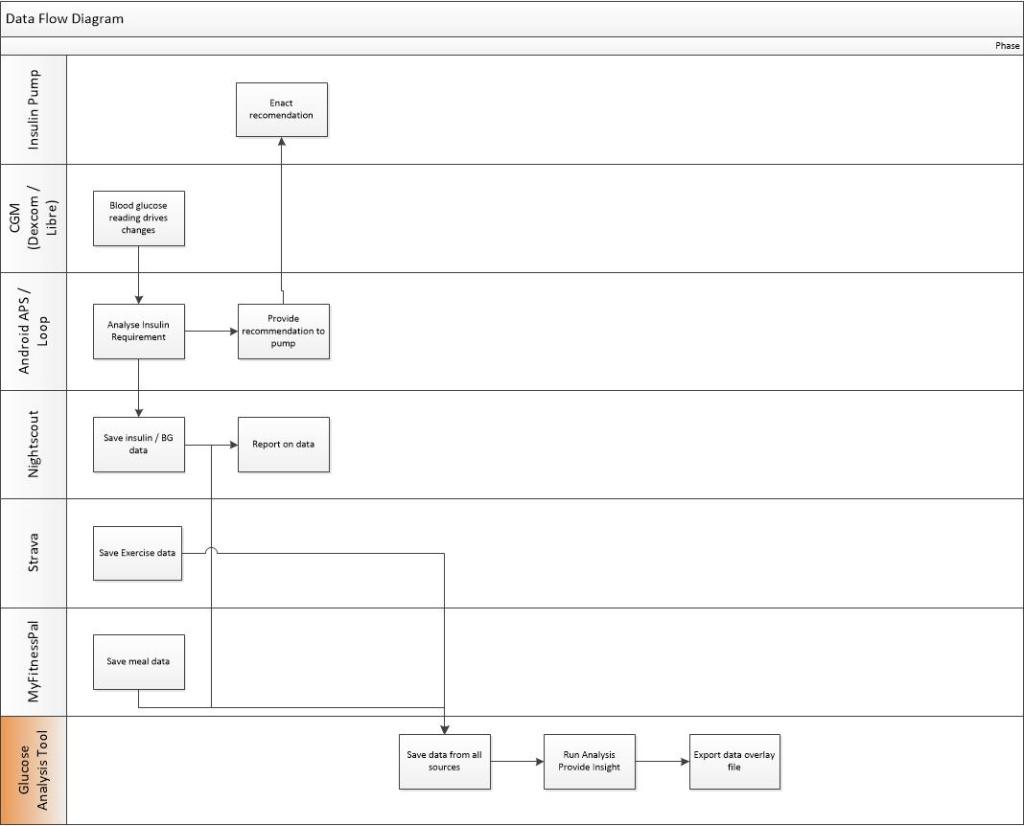
Goals
My goal was to provide some insight into what was working and was not. To do this I needed to obtain blood sugar readings as well as nutritional and exercise data. I achieved this by creating a tool that obtains data from Nightscout, Strava and MyFitnessPal This data is then processed and enriched to provide insight. I then developed a tool to export some of this data and display it on my YouTube videos. I had it connected to Garmin to extract sleep and exercise data but the Garmin API failed and I have not had time to update the program.
My tool will then do some analysis to provide some insight at a per meal or per activity level by looking at metrics like time-in-range, average glucose, standard deviation, max glucose, min glucose and many more metrics.
Below are some example’s of some of the data I am exporting and using to make decisions.
This tool is very much still under constant development, as I am always finding new stats to display and bugs with some of my current code (at present both the Garmin API and the MyFitnessPal API have issues)
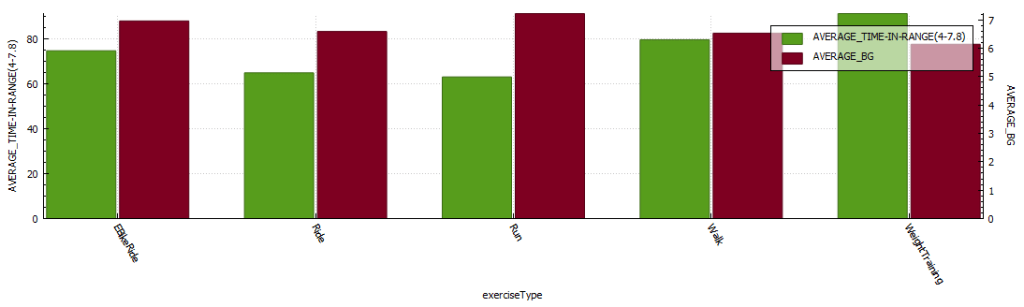
Below are some graphs and tables that I created in my Tool (The graphs are generated in DB Browser, these will at some stage be created in a JS library or Python graphing library).
Analysis of BG vs ISF, vs Sensitivity after a run.Analysis of BG vs ISF, vs Sensitivity after gym.Average TIR (time-in-range) and average blood glucose per exercise type for 2022.
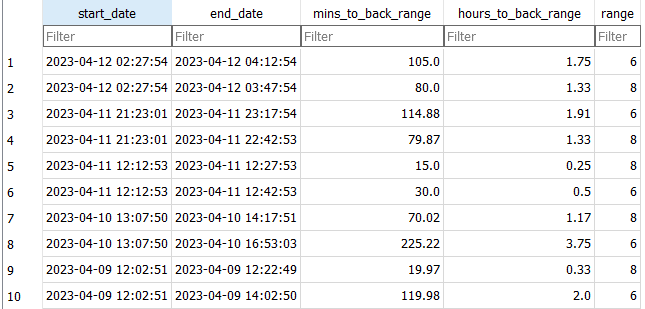
Return-to-Range
I use this table to understand how quickly the system is able to reduce sugars into a normal blood sugar range. At the moment I am using 8 and 6.
Return-to-range analysis (by year)
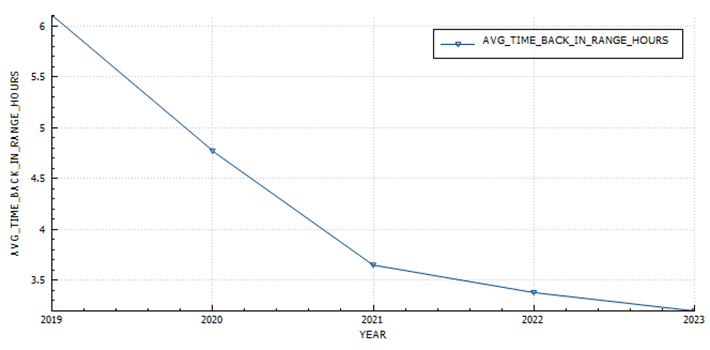
In 2019 It took just over 6 hours to return to euglycemia (blood glucose < 6) after a peak, in 2023 I managed to reduce that to 3.2 hours.
The average time it takes to return to a blood glucose of 6 mmol/l after a peak.
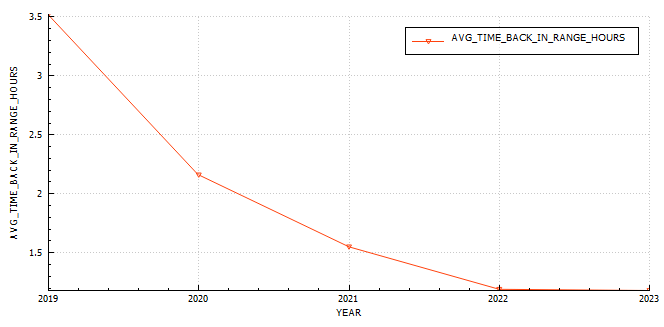
The average time it takes to return to a blood glucose of 8 mmol/l after a peak.
Daily Sensitivity Analysis
I find this useful to determine if I am more sensitive to insulin on certain days, usually due to exercise.
Exercise Sensitivity Analysis
The exercise sensitivity data has been updated to be hourly for 12 hours post exercise. Its now calculated via SQL (insert statement) and not a Python function into a staging table.
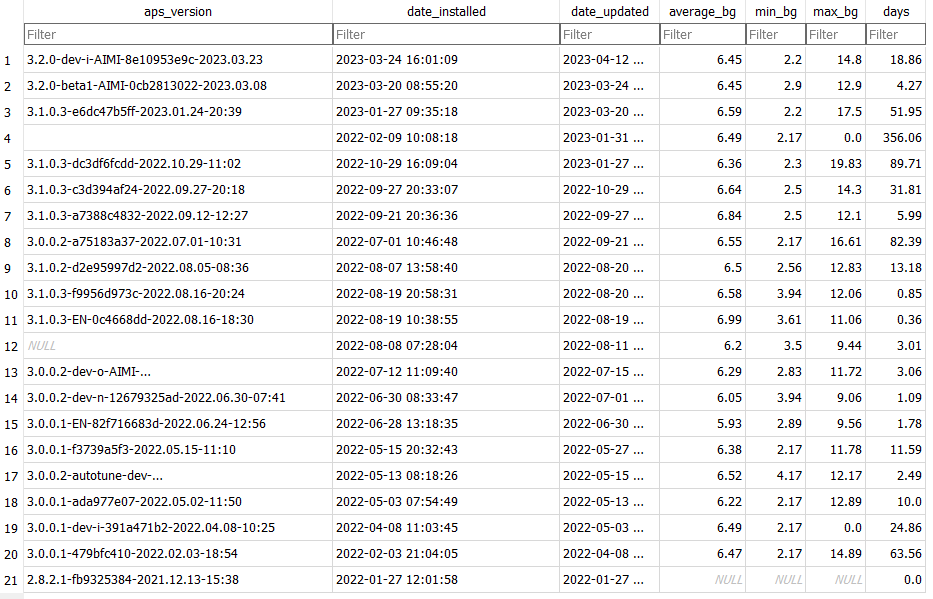
APS Version Analysis
APS Version Battery Analysis
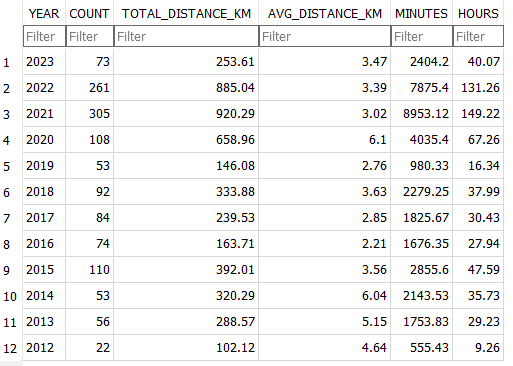
Exercise Stats Analysis (per exercise)
Exercise Stats Analysis (annual)
In the hopes of improving time-in-range while exercising I experimented with reducing insulin and used these values to provide insight into wether the changes were successful or not. In 2019 I was in-range only 66.6 of the time, in 2023 I am in-range 75%, with a slight improvement in glucose while exercising.
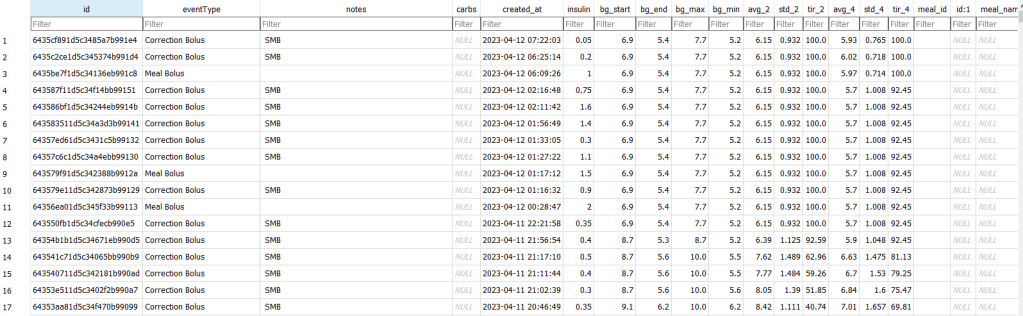
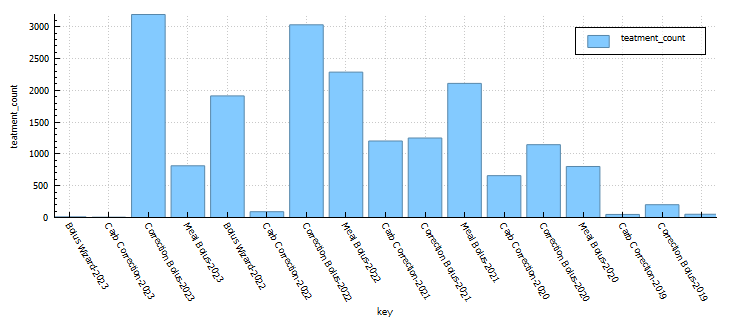
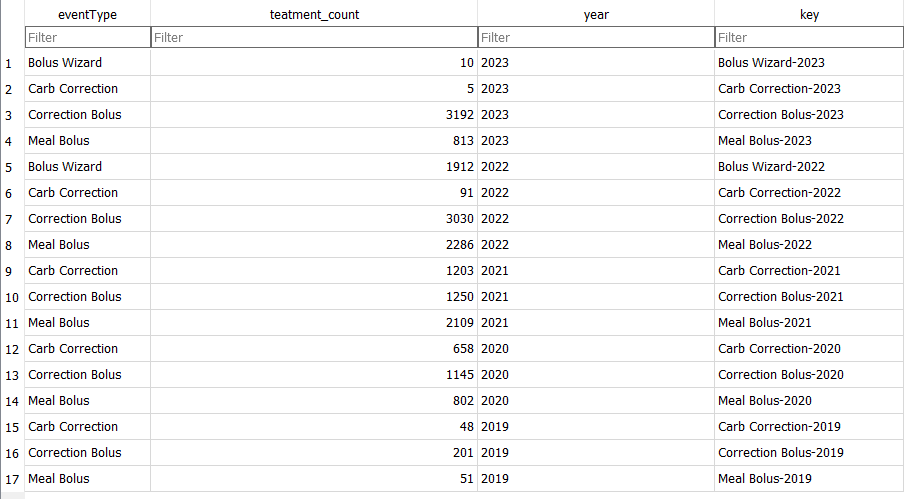
Treatments Analysis (per treatment)
Treatment Type Analysis
I use this table to understand how frequently I am interacting with the loop. This has little impact on the version of the variant of Android APS I am using.
Strava diabetic stats
I wanted to see diabetic statistics for each event in Strava, so I wrote a script to update the description field with some data I calculating in the Python tool. The script will check to see if the description field is populated and only update records that have no data in the description field.
It’s spring, and after a brief ‘almost two months’ of going off the reservation snacking at all times of day and barely exercising, I decided to check my weight. I discovered I had picked up a few kilograms since my last weigh in. After learning this, I decided that it was time for me to get my life back together and start another 30 day challenge. I find these great to provide the reason to get back into a routine.
I know that setting unrealistic goals (like losing 5kgs) isn’t going to work, so I’m going to break down my plan in to nutrition, exercise and diabetes goals.
Exercise
My plan for the month is to gym three days a week, run a minimum of 2 times per week and to mountain bike at least once a week. (So I guess I lied about setting unrealistic goals 🙂 )
Nutrition
For my meals I plan to stick to my usual low-ish carbohydrate meals during the week and try to only go coo-coo bananas on the late night snacking over the weekend. I’ll start carb-counting again as this will almost always yield the best results. This will be supplemented with 2-3 liters of water, depending on length of cardio that day.
Diabetes
Above is a chart of my starting metrics. Lets see how quickly I can improve those values. Its going to be a little bit of an unfair test as I was not carb-counting during the above period.
We want to see the In range (Time-in-range) increase and the standard deviation decrease. By doing that the average and the A1c should follow. This will mostly be achieved by the diet component of the plan. The exercise component will allow me to eat more cabs and require less insulin, as well as improve circulation, sleep, blood pressure, mood, cholesterol, memory and overall mental and physical health.
I will check in with weekly updates to ensure I keep motivated and accountable.