Is the new Coles low-carb bread type 1 diabetic friendly? Yes I think it is, read more below to discover why I think it is.
Review
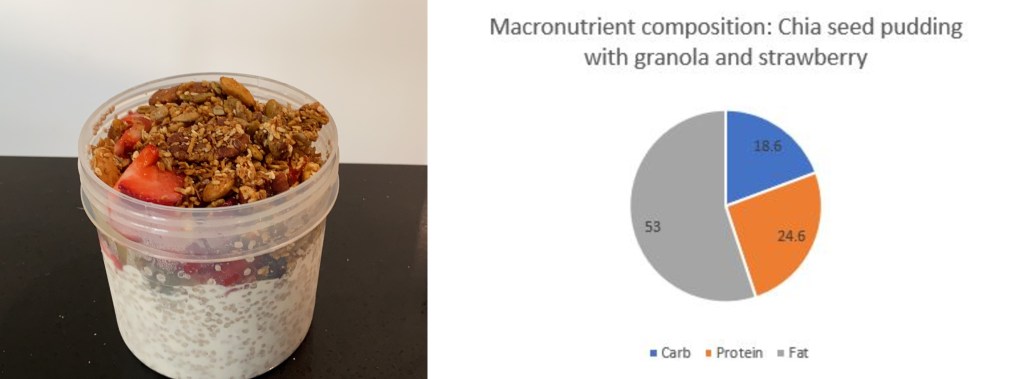
Nutritional Information
Insulin Strategy
Goal
Results
When trying anything new I always read the nutritional information on order to determine the impact it will have on my body. Certain high fat foods can cause insulin resistance and inflammation and will delay gastric emptying while protein will digest and get synthesised into carbohydrates.
Insulin Strategy
The strategy I used for this meal was based on the insulin type and macro composition. I injected for the carbs + (1/2 fibre) right before I ate as the Fiasp I use works almost immediately and so no pre-bolus was required. I then extended carbs at (protein*25%) + (fat *10%)
Goal:
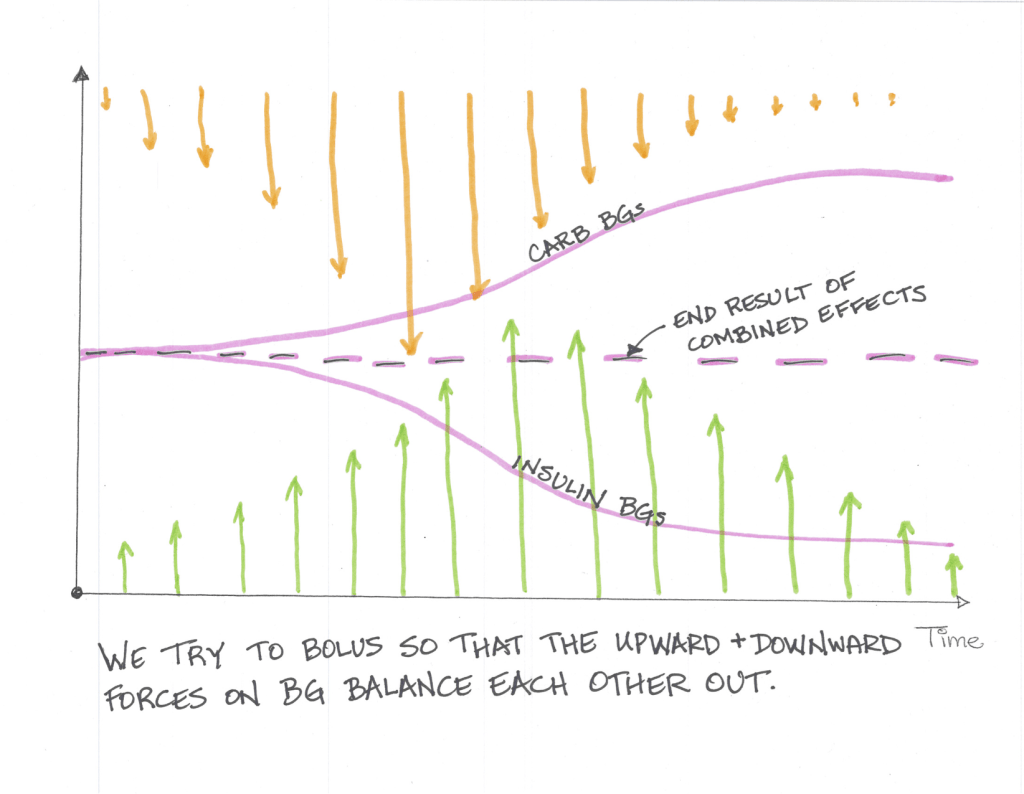
The goal of any insulin strategy would be to inject enough insulin at the correct time so that the upward force the carbohydrates exert is counteracted by the downward force the insulin exerts and you stay in range for the duration of the meal.
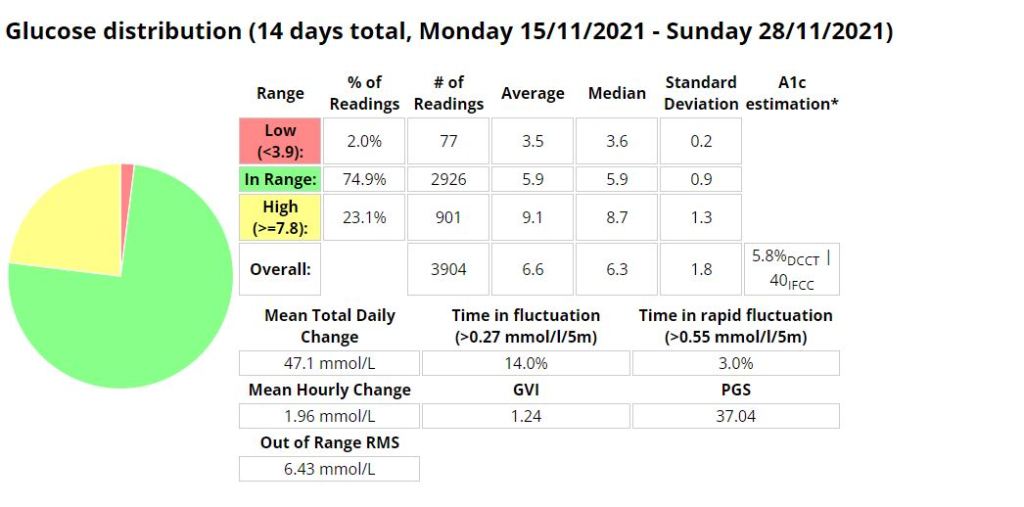
To analyse this I use three (3) values, standard deviation, time in range (TIR) and Coefficient of the variation. These three (3) values will assist you in determining how good or bad a meal was for you in terms of blood sugar impact (BGI).
Time in Range (TIR): For TIR we are looking for a high percentage of your readings within a normal (I use 3.9-7.8 mmol/l ) range.
Standard Deviation: For standard deviation I look for values under 1 as a meal that has little to no blood glucose impact (BGI).
Coefficient of the variation (CV): Is the standard deviation divided by the average glucose. Its a measure that helps normalise the results by reducing the influence on average glucose. Most studies indicate that anything under 33% is good.
Results:
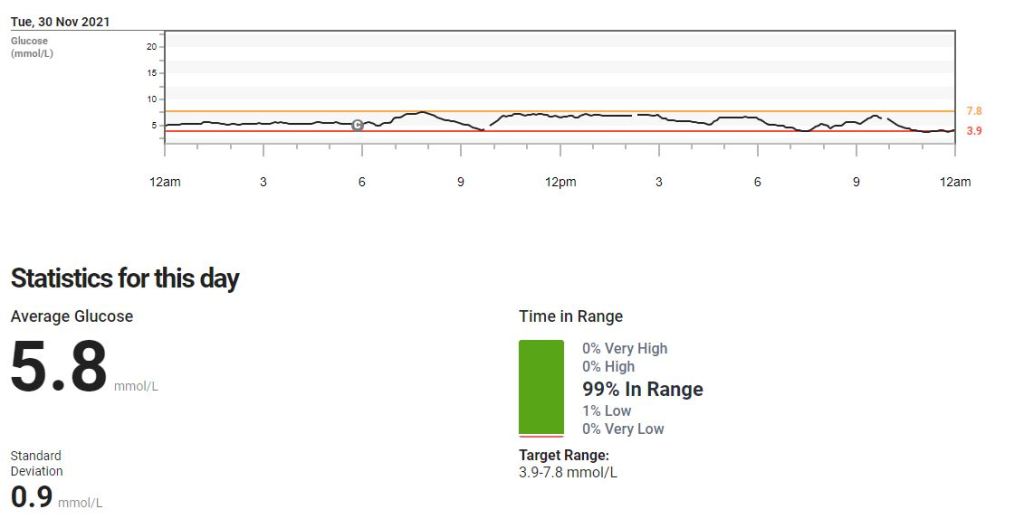
As we can see in the table below, the low-carb bread paired with the correct insulin strategy resulted in very stable blood sugars over a number of hours.
Time in Range (TIR): 100% (average)
Standard Deviation (SD): .5 (average)
Coefficient of the Variation (CV): 10% (average)
Read my post on some common foods I eat to gain a better understanding of how this meal impacted me in comparison.
Disclaimer: The information contained within this blog post are my thoughts and do not constitute medical advice. Please consult your medical team before making any changes to your diet or program.
This guide is based on past experience, information obtained from other diabetics and input from a multitude of websites.
I have broken this guide up into 3 sections;
Pre-exercise (preparation)
Exercise
Post-exercise
Step 1: Pre-exercise
PUMP: BASAL: If you are on a pump, this usually involves setting a temp basal around an hour prior to exercise, but a multitude of factors will govern the % basal rate and how early you will start it. It seems a general rule of thumb is 30-70% depending on the intensity and duration of the exercise, the longer you exercise the more sensitive to insulin you will become. The faster (think Fiasp) your insulin responds to change, the shorter the waiting period prior to starting exercise could be. Short acting Insulin has a DIA (duration of insulin action) that usually lasts several hours (3-7ish), and any insulin you may have on-board (circulating within your body) will become more potent as you exercise, thus increasing the risk of a severe hypo.
MDI: BASAL: For most exercise under 40 minutes I would keep my basal the same and ensure I exercised in the morning, reducing the risk of a hypo by being fasted and by exercising during a period in time where we are more resistant to insulin. Of course you can exercise at any time you choose, but you need to be aware that if you did not adjust your basal according to your length and vigour of activity you are more likely to experience a hypo.
Snack and snack timing: If you exercise in the morning I prefer to exercise fasted provided the activity is under 40 minutes in duration. If the activity is over 40 minutes then I will have a small snack (under 15g of carbs) just before I set out. The carbohydrate requirements for individuals will differ according to your body composition (ie. smaller people require less fuel to achieve the same results as larger people would, or the more muscle you have the more fuel you will need). If I am exercising more than two hours after I woke up, I will require a snack to sustain me for the duration of the activity. I have found that 20-30 minutes after my snack seems to be my ideal time (snacks with higher protein / fat will digest more slowly than high carb snacks) to begin exercise. Its very much a process of monitoring and evaluating until you find what works for you.
Hypo treatments: Glucose, dextrose or sucrose in liquid form is by far the quickest and most precise way to treat an impending hypo. Its important to note that liquid is absorbed much faster than solid foods according to the Manhattan gastroenterology website. Ingesting solids foods during activity can result in post-exercise hyperglycaemia as the foods begin to digest soon after exercise stops.
“Exercise and digestion can be mutually exclusive. When you exercise, your body isn’t using its energy for digestion. Instead, it slows any digestion currently taking place so it can divert as much blood as it can to feed your muscles and your lungs.”
I use a Camelbak Podium bum bag to store my pump, glucose gels and Powerade.
Other items to consider:
Cannula placement; If the cannula is in the muscle group you plan to train, you may need to reduce basal further.
Sleep; If you are sleep deprived you may require more insulin.
Wake up period; If you are training within two hours of waking up, you may be more insulin resistant and require less pre-training fuel.
Pump suspension; If you suspended your pump you will need to consider the period of time that your pump is suspended as you will have missed that basal insulin.
Step 2: Exercise
In my opinion, the most important things to do whilst exercising is to monitor and respond as required. I take my blood sugar at 15 minute internals when doing cardio ( I have a CGM attached to me at all times, but I prefer to use blood as its more accurate), which as you become more comfortable and attuned to your body, you could probably push to between 30 and 60 minutes to match testing to glycogen store depletion.
The average non-diabetic athlete has between 350-500g of stored glycogen when fully stocked (think high carb diets, the body stores less on lower carb diets) and up and 50% less glycogen just after waking up. These glycogen stores get fully depleted at around 90 minutes or 45 minutes if you exercise in the mornings . A Medivizor study suggested that diabetics have up to 21% less glycogen stores than the average person. If we consider the aforementioned statement regarding diabetics reduced capacity to store glycogen we realise that early morning exercise could lead to glycogen stores being depleted in as little as 35 minutes for the athletic individual, earlier if you are on a low carb diet or are untrained as your body uses glycogen less efficiently.
The Portland clinic advises that;
“During the first 15 minutes of exercise most of the sugar for fuel comes from either the blood stream or the muscle glycogen which is converted back to sugar. After 15 minutes of exercise, however, the fuel starts to come more from the glycogen stored in the liver. After 30 minutes of exercise, the body begins to get more of its energy from the free fatty acids”.
My personal experience seems to correlate to these findings and that’s why I test at 15 minute intervals, especially when starting a new routine, or restarting an old one. Also consider that you need insulin to utilise glycogen.
Effort levels can also influence blood glucose. Exercising at higher intensity levels can increase blood glucose due to stress hormones being released.
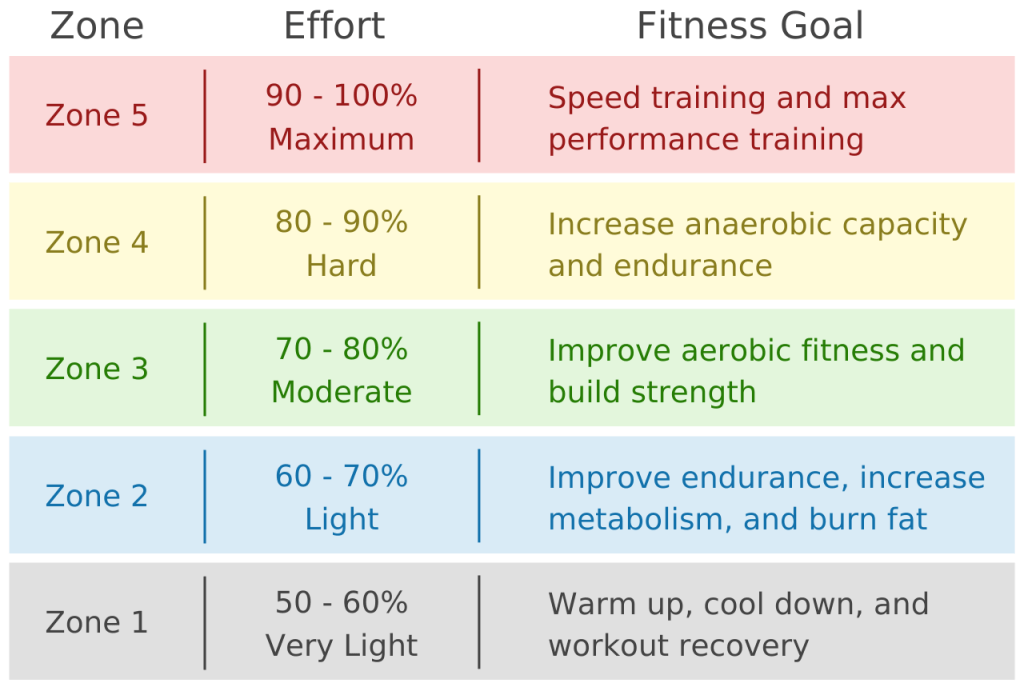
I use the formula 220-age to calculate my maximum heartrate. Then I can calculate effort from the below chart. I can then use this information to keep an eye on my heart rate during exercise and adjust my training effort as required. I also use this information to adjust my subsequent insulin doses as I am more sensitive to insulin an hour or two after exercise ( or directly post exercise when on MDI)
Starting Insulin recommendations in-line with activity durations
An example of how to use the table above would be if I had exercised at a moderate pace for 40 minutes, I could then experiment by decreasing my insulin dose by 67% and adjusting further if needed. Its easy to do this in Loop with temporary over-rides.
Temporary over-ride in Loop
An example of what I do to prepare for a run with Android Artificial Pancreas System (AAPS).
Step 3: Post Exercise
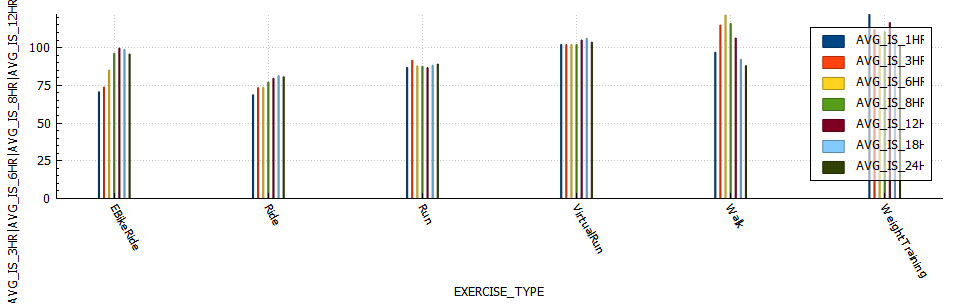
PUMP: I am not experiencing the sudden insulin sensitivity increase I did while on MDI. I believe this to be due to the fact that on MDI I cant reduce basal, but with the pump I can decrease basal as required. Be careful not to decrease your basal too much as your blood sugar will increase due to an inability to utilise glucose effectively. If you are using Loop then you could start a temporary over-ride to adjust insulin delivery for the remainder of the day. AAPS is capable of adjusting insulin requirements using a function called autosens which monitors deviations in insulin requirement. Below is a chart of insulin sensitivity post exercise grouped by exercise type.
MDI: I would generally be around 40% more sensitive to insulin immediately after a moderate run or cycle. This reason the onset of the sensitivity seems more rapid is due to the already circulating basal insulin now being super-charged. I found that exercising on MDI lacks some of the flexibility that pumps users have to adjust training duration or time period around your basal dose. On MDI I would the Spike app to adjust my meal time doses according according to the duration and intensity of the exercise. Spike is a very handy app for Apple MDI users to use as it can track meals, insulin and exercise. As well as have the functionality to calculate and adjust adjust insulin doses based on carbs and exercise input.
Screen capture of the the Spike-app.
NOTE: The Spike app is still available, it just requires a developer license and a significant time investment to install as its not available on test flight or the Apple store.
I am finally starting to return back to normality after starting to pump/Loop. Its taken a few weeks of focusing my efforts on running to gain the experience I wanted to acquire in terms of keeping myself mostly in range while I exercise, so I feel like its time to shift my focus towards cycling and gym again.
Gym (resistance training)
The first gym session back was mostly good, the only issue being Dexcom not registering a pretty severe (2.9 mmol/l) hypo. My body would usually register a hypo way in advance but I was pretty tired from the exercise.
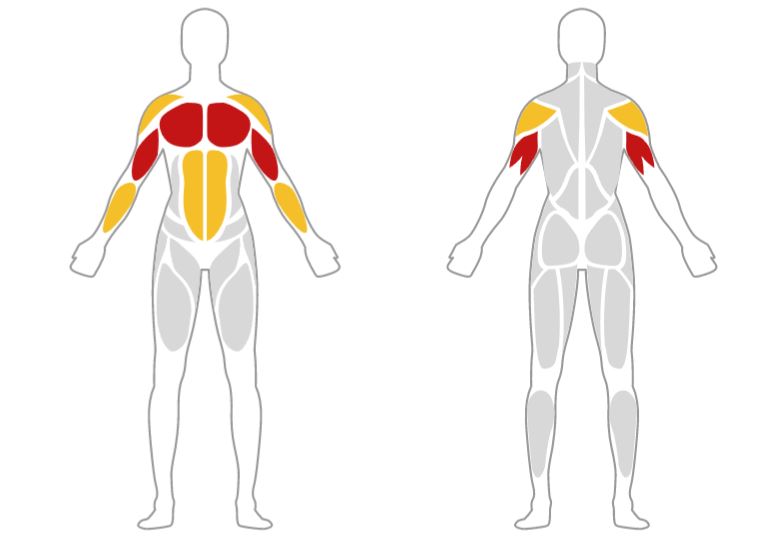
Muscles groups trained: Biceps / Triceps
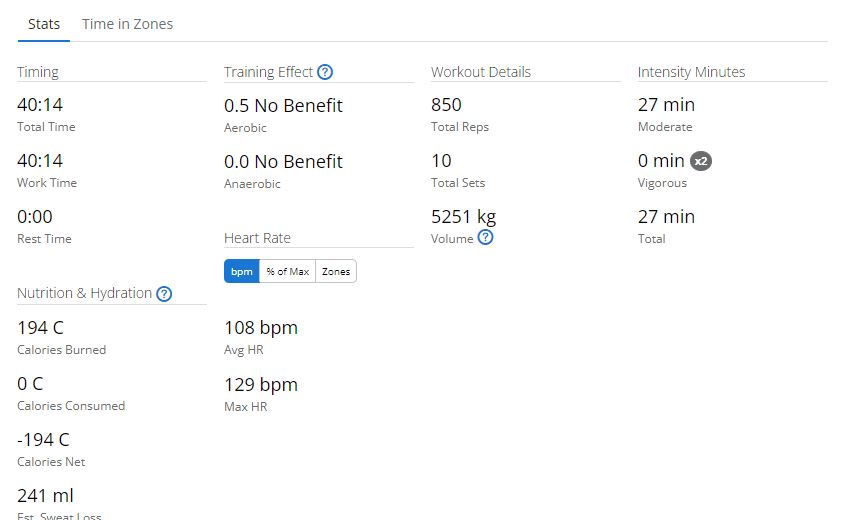
A gruelling 40 minutes with 5.2 Tons of weight being moved (at least according to Garmin’s calculation from me inputting exercise name and weight), which as expected is less than my last arm session where I moved 5.6 Tons. I’m fairly impressed I did as much as I did, as I was expecting much less.
December blood glucose stats
December 2021 Blood glucose stats are looking better.
My December update is quite pleasing. I am almost at 90% in range (3.9 – 7.8) and I am eating about 30% more carbs than I ate previously to achieve these numbers. I am not sure if I mentioned this before but I did a 30 day muscle building challenge about 3 months ago and one of the difficulties I experienced was eating more calories (to gain muscle) and staying in range. I am very happy with the 5.5% A1C and the standard deviation of 1.4. I would prefer to be 1 or under but with the introduction of more carbs that’s rather difficult to achieve at the moment.
I also wake up in range a lot more frequently these days. I am noticing a few more lows creeping in, perhaps a result of me needing to retune the Loop with the introduction of more frequent exercise?
Recently I feel as though my Dexcom is letting me down. I had two sensors fail back to back, which resulted me being without a CGM for a few days. Also Dexcom seems to be so delayed that by the time it alerts me of a hypo I have already corrected it in most cases. I am using the finger prick calibration method rather than the code calibration, which is supposed to be more accurate. Perhaps I need to adjust my calibration schedule to see if that helps.
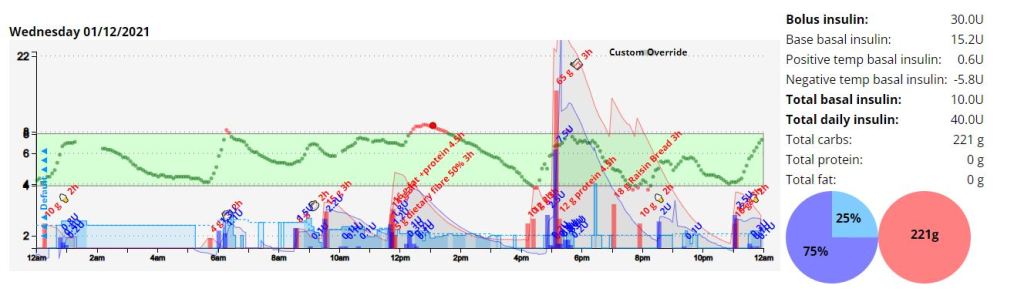
A few days ago I enabled micro-boluses in Free APS and its been working remarkably well at managing any post prandial blood sugars highs. I have only setup a 45% partial bolus being administered when deemed necessary, but at this stage I feel its performing as I want it to. I still count carbs and administer ‘fake’ or ‘extended’ carbs and simply use the micro-boluses as a tool to quickly administer insulin in place of an extended high temporary basal, which would do the job a little more slowly. Tonight I test this on Chinese food. 🙂
In the chart below we can see that I ate a hearty dinner, and then decided to eat some raisin toast. I managed to stay in range almost the entire evening after all these carbs. Amazing. I would never have even considered doing this before Loop, and if I did I would have anxiety the entire time.
UPDATE: The night went well and overall I am very happy with the results. If I am honest though, I think my expectation in the beginning of this experiment was that Loop would autonomously manage my blood sugar with very little input from myself, but I have realised and this is not the case, and adapted my management to include pre-emptive blood sugar correction. I am certain that Loop would indeed make these decisions, but keeping my finger on the pulse allows me to obtain the level of blood sugar control I am after.
Time-in-range (TIR) = >3.9 AND < 7.8mmol/l
The goal: Eat Chinese food and stay in range
The strategy: I went onto MyFitnessPal and found honey chicken, pork pieces and mixed veg. I added them into the dinner section and calculated the insulin required for the carbohydrate, protein and fat macros. I was not sold on the bolus amount for the carbs and ended up only injecting 70% of the calculated amount, but Loop quickly started administering micro-boluses to correct this. The ‘fake carbs’ ( I don’t really know why this name has gained so much traction in the diabetic community, since proteins and fats end up being synthesised into glucose (carbs) through gluconeogenesis, and are thus sugars (real carbs) being generated by the body at a slower rate than the exogenous carbs we eat) for protein and fat were then added to Loop with a 4.5 hour digestion period. This will allow Loop to attribute blood sugar changes to carbs (from gluconeogenesis) for up to 6 hours, and be able to micro-bolus or increase basal for them.
The outcome: I noticed that after an hour I had a substantial amount of insulin on-board and my blood glucose (BG) was dropping at a rate that could not be sustained by the food I had eaten, so I ate another 20g of faster acting carbs. An hour after that I had a mild hypo (3.7 mmol/l) and ended up eating again to correct this. I believe a better strategy may have been to inject 60% of the bolus up-front and then monitor for an hour before injecting the remaining bolus. Then again, this may have been just a carb-counting error on my part.
Improved time-in-range during exercise with decreased exercise anxiety
Lets start with A1C and Time-in-Range (TIR)
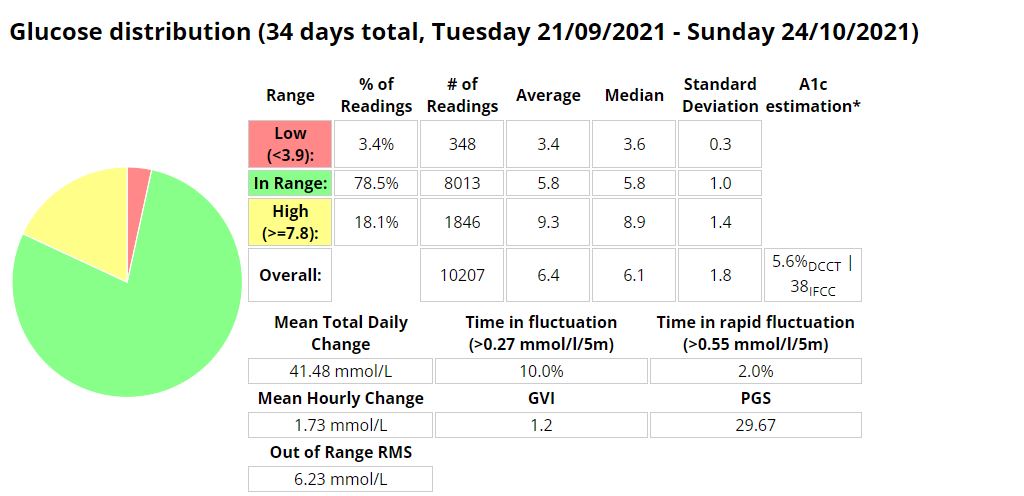
If we look at my stats just prior to looping, I had an A1C of 5.6% and a time-in-range (TIR) of 78.5%. The GVI and PGS stats were also really decent (more on these metrics here https://bionicwookiee.com/2020/02/26/cgm-metrics-gvi-pgs/), with a GVI of 1.2 (non-diabetic) and a PGS of 29 (non-diabetic). A decent average of 6.4 mmol/l, and 3.4 % (1h4min) of time in the 3.0 mmol/l – 3.9 mmol/l range.
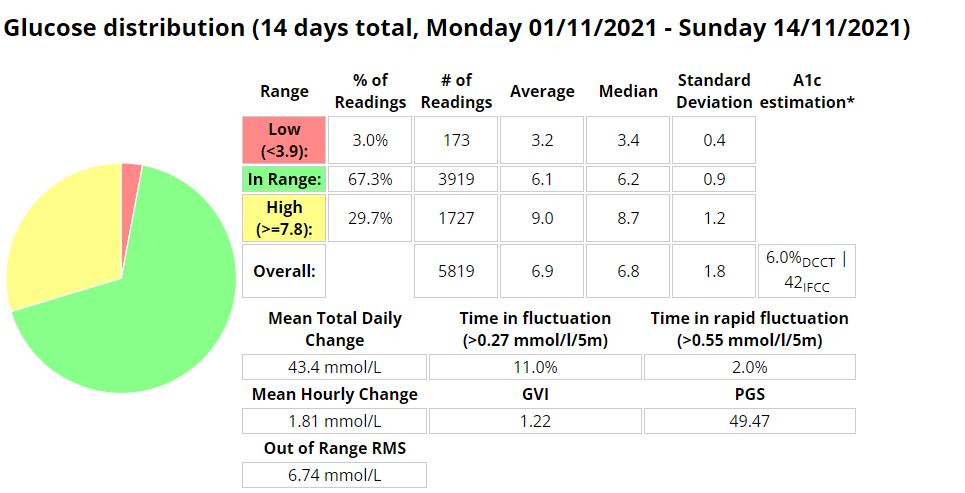
Now we look at my last month while on Loop. In order to reflect the learning curve involved from switching to a pump, I broke the stats into two (2) fortnightly blocks.
First two (2) weeks on LoopLast two (2) weeks on Loop
As can be seen in the charts above, some slight improvements are seen in all metrics discussed above with a 7.6% reduction in TIR and a 4.5% (-0.3) reduction in average blood glucose. The GVI and PGS metrics reflect modest variability and good control, as opposed to the previous non-diabetic results. I spent 22min (2%) in the 3-3.9 mmol/l range, down 10min from the previous periods 32min.
Reduce diabetic burden
This goal is subjective and difficult to quantify. Loop does make it easy to administer insulin, enable an over-ride, track carbohydrate absorption ( I was doing this with Spike) correct a hypo/hyper and even just wake up in-range. It does come with its own challenges and hurdles to overcome, like ensuring you have an up-to-date version, checking certificate expiry, ensuring your CGM is calibrated accurately, and then the challenges of constant site changes, reservoir and battery changes, insulin mixing and exercise.
Decrease food anxiety while increasing food options
It definitely feels like less of a burden to experiment with food or eat more carbs, as Loop can pick up any slack due to incorrect bolus calculations, or adjustments after exercise. I used to have 3.4 % (1h4min) hypos (3.0 mmol/l – 3.9 mmol/l) in a month due to incorrect dosing after exercise, but this number has significantly reduced to 2% (22min) while using Loop, as basal can be dynamically adjusted to fluctuations in blood glucose. Post prandial (meal) hyperglycaemia has also significantly been reduced, but I think in part due to Fiasp as it starts working immediately once injected.
MDI Average Carbs per day: 92.6 (*excluding ‘fake carbs’)
Loop Average Carbs per day: 121 (*including ‘fake carbs’)
*’Fake carbs’ are entered into Loop to manage the blood sugar spikes from gluconeogenesis (fat/protein synthesis into glucose)
Improve time-in-range (TIR) during exercise with decreased exercise anxiety
Unfortunately since switching to Loop the Python code I wrote to analyse blood glucose broke with the switch to Loop, so I only have the pre-loop analysis. I was quite happy with the control I had during exercise while on MDI.
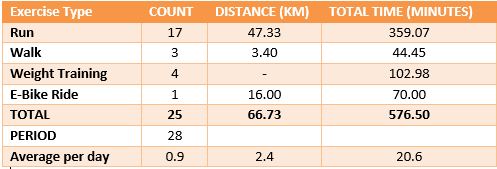
I have included the table I have been updating while I work on the Python code, which doesn’t seem to accurately reflect the amount of hypo events I have experienced while running. On the whole cardio has been the item on my list I have struggled with the most, and has been a significant source of anxiety. I am quite certain that after a few months I will have a strategy nailed down and the anxiety associated with exercise will wane. As can be seen in the below table, I am currently focusing on running as its the exercise I am struggling to gain control over the most. I was able to stay in range for the entire duration of all my weight sessions.
I’ll write a follow up post in the next month before I start my Android APS experiment. Good luck fellow Loopers!!
Last night went fairly well. The only big mistake I made was not injecting for protein/fat, but my guesstimates seemed to be pretty decent. Overall my weekly average is coming down, slowly but surely.